Adrian Becker - Orthodontic Treatment of Impacted Teeth
Здесь есть возможность читать онлайн «Adrian Becker - Orthodontic Treatment of Impacted Teeth» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Orthodontic Treatment of Impacted Teeth
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Orthodontic Treatment of Impacted Teeth: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Orthodontic Treatment of Impacted Teeth»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Provides protocols for common cases as well as complex and rare presentations Contains individual chapters on the specific aspects of the diagnosis and treatment of impaction in each of the different types of teeth Covers prevalence, etiology, diagnosis, attitudes to treatment, treatment timing, treatment methods, and prognosis Features more than 1,000 high-quality color images and illustrations
remains essential reading for all specialist orthodontists, academic researchers and instructors, oral and maxillofacial surgeons, and advanced students in orthodontics.
Orthodontic Treatment of Impacted Teeth — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Orthodontic Treatment of Impacted Teeth», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
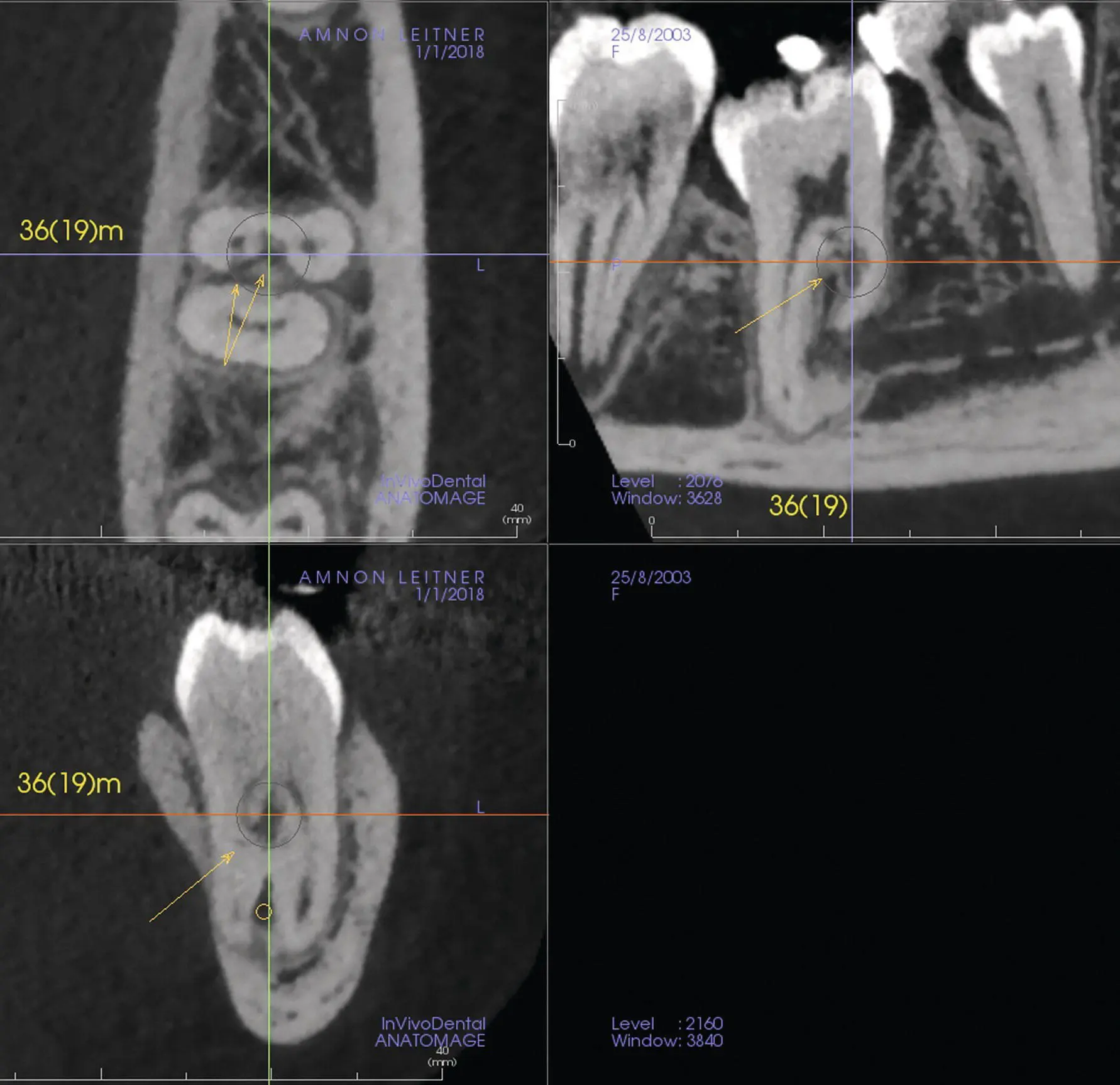
Fig. 4.21 Multi‐planar reconstruction view. Arrows indicate the invasive cervical root resorption lesion in the first molar mesial root.
The greatest advantage that the cone beam volumetric machine has over conventional CT machines is that its radiation dosage is only a fraction of that emitted by the medical machine. As shown in Table 4.1, the CBCT machine irradiates the patient at approximately 8–23% of the regular CT machine, when 8% is compared to small FOV and 23% compared to craniofacial (extra‐large) FOV.
Table 4.1is based on typical exposure protocols and is calculated from data collated from multiple published studies. The levels of standard 2D dental radiography, CT and CBCT patients’ median effective dose are compared and are shown as equivalent to daily background radiation. An average small FOV effective dose is 50 μSv, while that of a dental panoramic is about 20 μSv. A complete mouth series done with a round collimator ranges from 100 (CCD) to 200 (photostimulable phosphor plate, PSP) μSv.
What do these figures mean to the lay public? With our responsibility as dentists to convey information in a manner understandable to those seeking our treatment and in order to obtain informed consent, it is imperative to present the issue in its context, without blinding the patient with scientific data. Thus, it may be more pertinent to use the comparison that (a) the average person receives a dose of about 8 μSv per day or 2700 μSv per year from the environment [28]; and (b) flying from New York to Tokyo by the transpolar route exposes the passenger to ionizing (cosmic) X‐rays of approximately 150 μSv and from New York to Seattle approximately 60 μSv [29].CBCT represents state‐of‐the‐art technology, with direct relevance to the determination of macroscopic anatomy and accurate positional diagnosis of impacted teeth. The machinery is not beyond the financial means of most hospitals, radiology institutes, imaging centres, dental clinics and dental school radiology departments. Its advantages to the orthodontist and surgeon are manifest. Its level of emitted ionizing radiation is low and the cost to the patient affordable. It is a recommended procedure for many of the cases discussed within the context of this book.
Table 4.1 Typical effective dose from radiographic examination.
Source: Reproduced by kind permission of Dr S.M. Mallya and Elsevier Publishers.
| Examination | Median Effective Dose | Equivalent Background Exposure a |
|---|---|---|
| Intra‐oral b | ||
| Rectangular collimation | ||
| Posterior bite‐wings: PSP or F‐speed film | 5 μSv | 0.6 day |
| Full‐mouth: PSP or F‐speed film | 40 μSv | 5 days |
| Full‐mouth: CCD sensor (estimated) | 20 μSv | 2.5 days |
| Round collimation | ||
| Full‐mouth: D‐speed film | 400 μSv | 48 days |
| Full‐mouth: PSP or F‐speed film | 200 μSv | 24 days |
| Full‐mouth: CCD sensor (estimated) | 100 μSv | 12 days |
| Extra‐oral | ||
| Panoramic b | 20 μSv | 2.5 days |
| Cephalometric b | 5 μSv | 0.6 day |
| Chest c | 100 μSv | 12 days |
| Cone beam CT b | ||
| Small field of view (<6 cm) | 50 μSv | 6 days |
| Medium field of view (dentoalveolar, full arch) | 100 μSv | 12 days |
| Large field of view (craniofacial) | 120 μSv | 15 days |
| Multidetector CT | ||
| Maxillofacial b | 650 μSv | 2 months |
| Head c | 2 mSv | 8 months |
| Chest c | 7 mSv | 2 years |
| Abdomen and pelvis, with and without contrast c | 20 mSv | 7 years |
aApproximate equivalent background exposure is calculated based on an estimated background radiation dose of 3.1 mSv/year. Exposures more than the equivalent of 3 days are rounded off to the nearest day, month or year.
bMedian dose from dento‐maxillofacial radiography with typical exposure protocols is calculated from data collated from multiple published studies. Doses in the range of 10–1000 μSv are rounded off to the nearest multiple of 10.
cAmerican College of Radiology, https://www.acr.org/Clinical‐Resources/Radiology‐Safety/Radiation‐Safety.
CCD, charge‐coupled device; CT, computed tomography; PSP, photostimulable phosphor.
Having said that, however, there is an inherent danger with this type of comprehensive imaging. The means of presentation of the results of the CBCT scan are very attractive to the layperson and several of the animations may be undertaken to impress the orthodontic patient, who may request a copy of the ‘before and after’ portfolio as a souvenir of the orthodontic treatment and outcome. In today’s world, this can easily become part of the ‘hard sell’ and a means of attracting new patients. Consequently, the danger is that the stage may be set for the production of animations for the sake of ‘completeness’, much of which may be superfluous to the clinical needs of the patient, resulting in excess exposure of the patient to a large overdose of ionizing radiation.
ALARA
This leads us to explain the term ALARA – and what it means in practice [30].
It is only many years after treatment with any form of radiation that we see the stochastic effects, which include a higher susceptibility of the individual to various forms of cancer. It is known that these effects are amplified with increased exposure and that children are more susceptible than adults. Yet it is children and young adults who are the main patient population for orthodontic treatment. It is therefore incumbent on the practitioner to reduce this exposure to the minimum, while deriving a maximum of information adequate to the problem in hand. This is what ALARA signifies – As Low As Reasonably Achievable.
As we have already noted, there is a selection of scanning protocols and a low‐dose feature in every machine. It stands to reason, therefore, that when a CBCT scan is justified, it is because plane 2D radiography cannot maximize the information needed for that patient, or that dose risk/benefit weighs in favour of CBCT. CBCT should be performed using the scanning protocol with the most efficacious risk/benefit and the smallest FOV possible.
Unfortunately, most orthodontists are not exploiting all the benefits of the CBCT scan, despite the fact that they tend either to scan patients in‐house or refer them to an imaging centre, or to a colleague who has the facilities and the know‐how available. It is of paramount importance that this wanton and cavalier attitude to CBCT scans should be disparaged and be replaced by orthodontists themselves becoming familiar with the important advantages offered by these machines.
In order to fulfil optimal scanning requirements for accurate diagnosis, orthodontists must be involved, proactive and specific regarding FOV and all other scanning parameters, including for such simple and apparently trivial instructions as scanning a seated patient, even with machines designed for erect subjects. All video animations prepared and produced by Amnon Leitner (panorama@inter.net.il).
References
1 1. Seward GR. Radiology in general practice IX. Unerupted maxillary canines, central incisors and supernumeraries. Br Dent J 1968; 115: 85–91.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Orthodontic Treatment of Impacted Teeth»
Представляем Вашему вниманию похожие книги на «Orthodontic Treatment of Impacted Teeth» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.


Обсуждение, отзывы о книге «Orthodontic Treatment of Impacted Teeth» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.