Adrian Becker - Orthodontic Treatment of Impacted Teeth
Здесь есть возможность читать онлайн «Adrian Becker - Orthodontic Treatment of Impacted Teeth» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Orthodontic Treatment of Impacted Teeth
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Orthodontic Treatment of Impacted Teeth: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Orthodontic Treatment of Impacted Teeth»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Provides protocols for common cases as well as complex and rare presentations Contains individual chapters on the specific aspects of the diagnosis and treatment of impaction in each of the different types of teeth Covers prevalence, etiology, diagnosis, attitudes to treatment, treatment timing, treatment methods, and prognosis Features more than 1,000 high-quality color images and illustrations
remains essential reading for all specialist orthodontists, academic researchers and instructors, oral and maxillofacial surgeons, and advanced students in orthodontics.
Orthodontic Treatment of Impacted Teeth — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Orthodontic Treatment of Impacted Teeth», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Orthodontists generally use elastic ligatures and chains to move teeth by tying the material in its stretched, elongated form, thereby drawing the dental elements towards one another. However, the range of elasticity in this longitudinal direction will be limited and, as pointed out above, will decay rapidly. Nevertheless, a lateral displacement of an elongated elastic thread produces a potentially greater range of movement, within suitable orthodontic force levels, than does a longitudinal displacement. This ‘slingshot’ principle may be more efficiently applied to move teeth that lie at a distance from the main arch, giving more controlled and measurable forces ( Figure 2.7a, b).
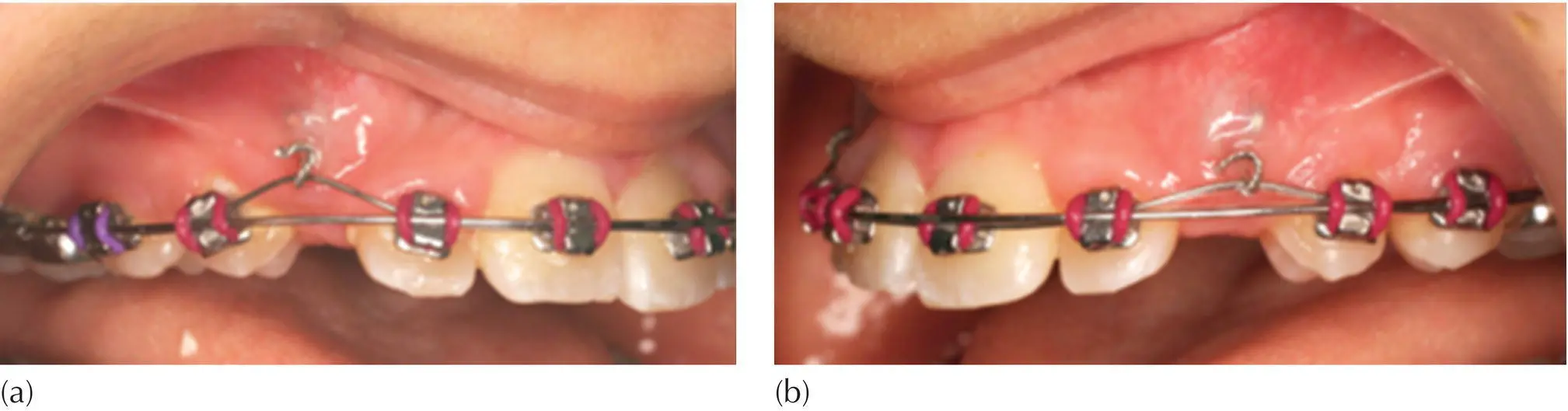
Fig. 2.7 (a, b) The use of nickel–titanium auxiliary wire as the active element in applying eruptive force to the unerupted canines, by being thread through the ‘rolled‐up’ stainless steel pigtails that are ligated to the eyelets. There is a heavy 0.020 in. gauge base arch. The low‐profile eyelets, which were bonded at exposure in a closed surgery procedure, can be seen through the translucency of the healthy and uninflamed gingiva.
Notwithstanding these comments and with the required careful consideration in the planning of their use, elastic ties, nickel–titanium auxiliary archwires, chains and modules are extremely helpful in many situations created by the presence of impacted teeth. However, properly designed springs, auxiliary to a heavy base arch, are usually more efficient: they are able to deliver a measured and controlled force, the force decay is lower, a variety of metallic alloys are available for spring fabrication, their range of action may be very broad and their direction is accurate. These will be illustrated in the succeeding chapters in the consideration of cases as they pertain to the individual groups of teeth.
Thus far, our discussion has centred on maintenance of a steady force through as wide a range as possible. Now we must address the force values that are appropriate for application to an impacted tooth.
When planning traction to a single‐rooted tooth through its long axis, pure extrusion is produced with no resistance from the bone of the coronally divergent socket. Thus, the force is applied to the tooth and transferred directly to the supporting fibres of the PDL. As such it requires to be minimal – of the order of 10–15 g – because resistance is small. If a greater force is applied, the tooth may become excessively loose and the extrusion achieved will bring with it relatively little supporting alveolar bone.
If we then introduce a modicum of tip into this movement, then the tooth will be brought into close proximity with the bony socket walls, thus interjecting resistance. Compressing the fibres on the pressure side and stretching them on the tension side will generate hyalinization and cause undermining resorption of the alveolar bone. The force required to elicit eruption will be in the range of 20–40 g/cm 2of root surface.
Soft tissue resistance must also be taken into consideration. With a simple window technique exposure, the crown of the tooth is free to erupt directly to its place, with little or no interference from the soft tissues. The full traction force is transmitted to the PDL at the cementum/alveolar bone interface. By contrast, a closed eruption technique will leave the tooth covered by a soft tissue flap, which will have been firmly sutured into its former place. Some of the applied traction will then be dissipated in overcoming the tension of this soft tissue flap and must therefore be increased to reach the threshold needed for tooth movement.
When traction is applied to a tooth following an apically repositioned flap procedure, tension is created in the tissues by virtue of the fact that the flap has been sutured superiorly to the labial side of the tooth. This tension is eruptively directed and may then cumulatively magnify the applied force. For this reason, it is sometimes advisable in the first instance to rely only on pressure from the sutured flap, leaving the application of biomechanical traction to a subsequent visit. This is particularly relevant in cases where the tooth is high and labially or buccally displaced.
Temporary anchorage devices
Bone anchor screw
Treating impacted teeth largely has to do with the facility to develop vertical eruptive forces and to bring them to bear on ‘vertically challenged’ teeth. At best, there is very little bone in the same jaw coronal to an impacted tooth at the outset, and certainly less or none after the tooth has been surgically exposed. This leaves precious little opportunity to establish an ‘anchor’ against which to tie elastic modules and chains for the horizontal movement of teeth in various directions [19, 20]. As a means of obtaining skeletal anchorage, a simple titanium screw temporary implant is often used in routine orthodontics. A screw device is placed as the base, to which traction may be applied from a small distance to attempt to obtain an appreciable range of action.
In this limited sense, therefore, using a temporary anchorage device (TAD) in the same jaw as the impacted tooth is largely inappropriate. Some of these screws are designed with two slots at right‐angles to one another, which serve as the means for driving the screw into the bone, but may also be used as an orthodontic bracket slot into which a rectangular archwire may be ligated in the usual manner. Other designs include a slot for an orthodontic archwire in the neck of the screw, beneath the screw head. A short length of rectangular 0.019 in. × 0.025 in. wire may be fabricated into a custom‐made, self‐supported spring. This is then rigidly tied into the slot on the screw, which will have been placed at some distance and in a more convenient mesial, distal or apical location in relation to the impacted tooth. The screw (the anchor) may then be used as a platform from which to apply traction to the tooth and to erupt it vertically to a considerable degree.
Using a TAD as a direct anchor in the opposite jaw, in the absence of an orthodontic appliance, has the clear advantage that there can be no adverse (particularly intrusive) movement of the teeth adjacent to the impacted tooth, since these are not exploited as anchor units. Nevertheless, this method demands the cooperation of the patient in the placement of intermaxillary elastics, stretching from the device to the pigtail ligature hook, which itself extends from the bonded orthodontic bracket/button/eyelet on the impacted tooth. These two rigid extremities on which to place the elastic are not always easily accessible for the patient or even for a dedicated parent, and may accordingly prove to be impractical in some cases. To circumvent this problem, it will be necessary to place a full orthodontic appliance, which is stabilized by ligation to a TAD on the affected side in the opposing dental arch. This provides an implant‐supported anchor arch configuration. Intermaxillary traction from any conveniently located hook or bracket on that appliance may then be applied directly to the attachment on the impacted tooth, without fear that the teeth in the anchor arch will over‐erupt. This will also assume that the attachment hook on the impacted tooth is accessible for the patient and is not painful to manipulate.
Impacted second molars, which are largely inaccessible for the patient, require a more circuitous approach. This approach dictates setting up the same implant‐supported configuration in the opposing anchor arch, but in this case a full appliance also needs to be placed in the affected arch.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Orthodontic Treatment of Impacted Teeth»
Представляем Вашему вниманию похожие книги на «Orthodontic Treatment of Impacted Teeth» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.


Обсуждение, отзывы о книге «Orthodontic Treatment of Impacted Teeth» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.