Adrian Becker - Orthodontic Treatment of Impacted Teeth
Здесь есть возможность читать онлайн «Adrian Becker - Orthodontic Treatment of Impacted Teeth» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Orthodontic Treatment of Impacted Teeth
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Orthodontic Treatment of Impacted Teeth: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Orthodontic Treatment of Impacted Teeth»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Provides protocols for common cases as well as complex and rare presentations Contains individual chapters on the specific aspects of the diagnosis and treatment of impaction in each of the different types of teeth Covers prevalence, etiology, diagnosis, attitudes to treatment, treatment timing, treatment methods, and prognosis Features more than 1,000 high-quality color images and illustrations
remains essential reading for all specialist orthodontists, academic researchers and instructors, oral and maxillofacial surgeons, and advanced students in orthodontics.
Orthodontic Treatment of Impacted Teeth — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Orthodontic Treatment of Impacted Teeth», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
The particular stage of the initial movement of the impacted tooth, from its ectopic position until it reaches the main archwire, effectively represents the resolution of the impaction. This entire stage, until the bonded attachment arrives at and engages the main archwire, is the most difficult part of the treatment of the displaced tooth and it is not possible to achieve much more than tipping, extrusion and some rotation. In other words, the value of the bracket up to that point is no greater than that of a simple eyelet [14]. Indeed, on several counts, the potential of the eyelet outweighs that of the conventional bracket during the impaction resolution stage.
The base of a conventional bracket is wide and rigid and is manufactured so as to closely conform to the shape of the crown of the tooth in its mid‐buccal location. It is impossible to adapt this preformed base to the shape of another part of the tooth’s surface than that ‘average, one‐size‐and‐shape‐fits‐all’ contour for which it has been designed. It follows that composite bonding on a different location on the tooth is very likely to lead to failure [14]. Orthodontic brackets are highly specialized, each having a slot milled to a very precise blueprint, specific to the particular tooth for which it is intended. The mesio‐distal angulation differs between one tooth and another, the ‘in–out’ bucco‐lingual depth of the slot will vary, the torque angulation will not be the same for all the individual teeth, and the height at which the bracket should be placed on an incisor will not be the same as that on the canine. These are the basic definitions on which the so‐called straight‐wire appliances are built. Accordingly, it is quite obvious that all this highly sophisticated programmed engineering is only meaningful if the bracket is bonded in its appropriate, predetermined mid‐buccal location on the crown of the tooth. We shall see in later chapters that, at the time of the surgical exposure of an impacted tooth, it is very frequently logistically impossible or inadvisable to bond an attachment in the mid‐buccal position on the crown. This site on the crown of the tooth may not be accessible due to its relationship to the root of an adjacent tooth. An excessive amount of soft and hard tissue might need to be surgically removed in order to provide access to achieve the ideal placement, thereby producing unnecessary surgical damage, which always has a price to pay in the form of appearance and long‐term periodontal prognosis of the treated result [14].
The standard orthodontic bracket in any technique is relatively large, possesses a wide, high and sharp profile, and, even when placed in alternative positions on the tooth (by force of circumstance at the time of surgery), may find itself deeply sited within the surgical wound. The shear bulk of the bracket creates irritation as the tooth is later drawn through the soft tissues, particularly the mucosa ( Figure 2.3). A ligature wire or elastic thread, which will have been tied to it, must also originate deep in the wound and will be stretched across the replaced flap tissue in the direction of the labial archwire. This will increase the possibility of impingement of the investing tissues and may lead to inflammation and even to permanent periodontal damage.

Fig. 2.3 As the impacted tooth is about to erupt, the high‐profile Siamese edgewise bracket has fenestrated the swollen gingival tissue.
As the displaced tooth moves towards its place in the arch, exuberant gingival tissue bunches up in front of it, leading to a confrontation with a conventional orthodontic bracket. The existence of the exuberant gingival tissue in advance of the tooth can often cause ‘pinching’ between this tissue and the teeth in the arch immediately adjacent to it. This is less likely to occur if a deliberately generous space has been previously provided in the arch for the tooth. Such a precaution may avoid unnecessary periodontal damage.
A simple eyelet or button
An eyelet, welded to orthodontic bond material with a mesh backing ( Figure 2.4), is soft and easy to contour, enabling its adaptation to the bonding surface to be more intimate and retentive. Its relatively small size and low profile make the mid‐buccal position of several of the more awkwardly placed teeth considerably more accessible as compared with the placing of a conventional bracket. Its modest dimensions are also less of an irritant to the surrounding tissues, particularly during the critical phase as it breaks through gingival tissues in the final stages of its eruption into the oral cavity [15].
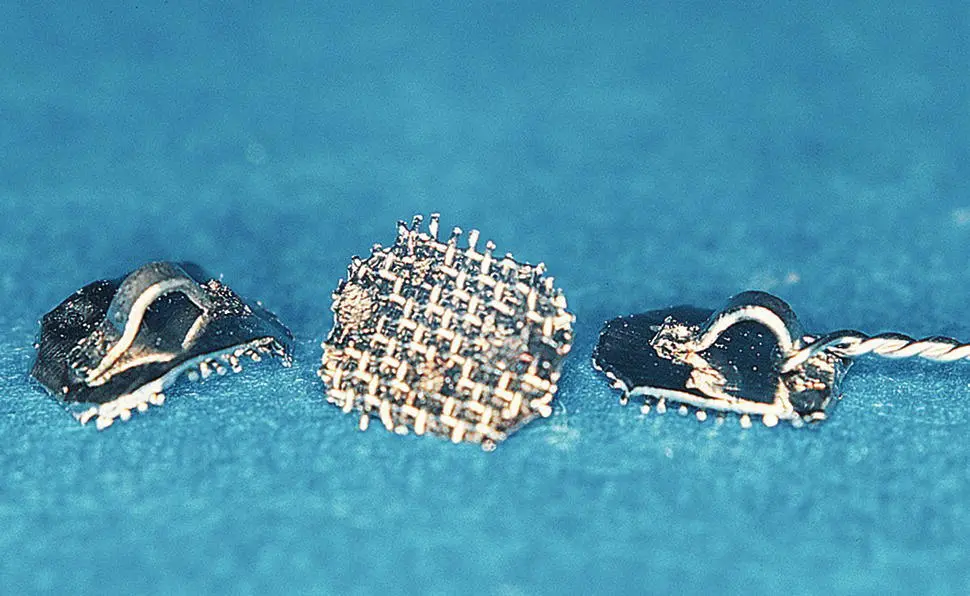
Fig. 2.4 Eyelets welded to a pliable band material base, backed by steel mesh.
The need to properly adapt the base of the attachment to the shape of the recipient surface of the crown of the tooth cannot be over‐emphasized. Thus, the use of standard brackets with ‘anatomic’ bases, as supplied by the manufacturer, has been shown [14] to fare considerably better in the mid‐buccal position of the impacted tooth (80.6%) than on any other surface, particularly the palatal surface. The chances of the survival on a palatal site were shown to be 58.3% – i.e. a failure rate of almost 1 in 2. By comparison, a small attachment (such as an eyelet) on a pliable base, properly and individually adapted to the form of the recipient site, which demonstrated a 96.7% level of reliability against detachment, will allow the orthodontist to work with the greatest degree of confidence.
A button is useful for engaging elastic chains and is usually placed on the lingual side of a tooth in circumstances where rotation of the tooth is required. However, it is also suitable in the present context.
For these reasons, small eyelets and buttons are recommended as the initial attachment, which is placed at the time of surgery and removed only when the tooth has progressed to the point where it is in close proximity to the archwire. At that point in time, they should be replaced by the same type of sophisticated bracket that is being used on the other teeth, thereby initiating the more intricate root manipulations of the tooth (rotating, uprighting and torqueing). Also at this point, the impaction will have been treated and there will be no ectopically displaced teeth. All the teeth will be located close to the line of the arches, forming what would otherwise constitute a typical pre‐orthodontic scenario. Elsewhere in this book I have called this environment the ‘orthodontic ballpark’, because the case will have now become a routine orthodontic case.
Intermediaries/connectors
We shall see in Chapter 4and again in Chapters 6and 7that there are important periodontal advantages to be gained by full closure of the surgical flap at the end of the visit at which the surgical exposure is performed [15]. The impacted tooth will have been re‐covered by the surgical flap and will be lost from sight, unless the impacted tooth is fairly superficially placed. The only manner in which contact may be maintained with it is through some form of physical connection, such as a ligature wire, gold chain or elastic thread, which was attached to the eyelet before or immediately after it was bonded to the tooth. These may be termed intermediaries or connectors.
Since elastic thread can only be tied once, it is not recommended to be used as an intermediary. Gold chain has found a surprising degree of acclaim and acceptance worldwide because it is undoubtedly suitable and sufficiently strong to serve as an intermediary. However, it is unnecessarily sophisticated, expensive and not widely available. There is also one practical drawback to its use, which relates to its physical properties. If a closed surgical approach is used after bonding of its attachment base to a tooth, the end of the chain will need to be held in locking tweezers or artery forceps until it is ligated to its active traction element, be it a spring or elastic thread. If the gold chain is not thus held, then the fine‐linked chain may collapse down and slip between the recently sutured edges of the flaps and be lost from sight. This may also happen when an open surgical approach is performed, where the collapsed chain may fall between the wound edges and into the cervical area of the newly exposed tooth. Indeed, this entire unfortunate series of events may also occur during later visits for re‐ligation of the still only partially erupted tooth. In all the above cases, the subsequent search for the lost chain is very uncomfortable for the patient and may even require reopening of the healing soft tissue cover.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Orthodontic Treatment of Impacted Teeth»
Представляем Вашему вниманию похожие книги на «Orthodontic Treatment of Impacted Teeth» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.


Обсуждение, отзывы о книге «Orthodontic Treatment of Impacted Teeth» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.