Veterinary Surgical Oncology
Здесь есть возможность читать онлайн «Veterinary Surgical Oncology» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Veterinary Surgical Oncology
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Veterinary Surgical Oncology: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Veterinary Surgical Oncology»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
The new edition of the most comprehensive resource on surgical oncology, covering both basic and advanced surgical oncology procedures in small animals Veterinary Surgical Oncology
Veterinary Surgical Oncology
Veterinary Surgical Oncology, Second Edition
Veterinary Surgical Oncology — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Veterinary Surgical Oncology», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Instrumentation includes a #10 or #15 blade, Metzenbaum scissors, forceps, Mayo scissors, and suture. The surgical site is clipped free of fur, and the patient is prepared with aseptic technique and draped. An incision slightly larger than the palpable lymph node is made parallel to the axis of the lymph node. The superficial tissue overlying the lymph node is bluntly and sharply dissected. The lymph node capsule is then grasped with the forceps and blunt and/or sharp dissection is performed around the lymph node to free it from the surrounding tissue. Vessels that are encountered may need to be ligated. The lymph node is then removed, and the subcutaneous tissue and skin are closed. Many “lymph nodes” are actually lymphocenters. The implication is that multiple lymph nodes can be present in one location, for example, the mandibular lymphocenter often has two to three lymph nodes.
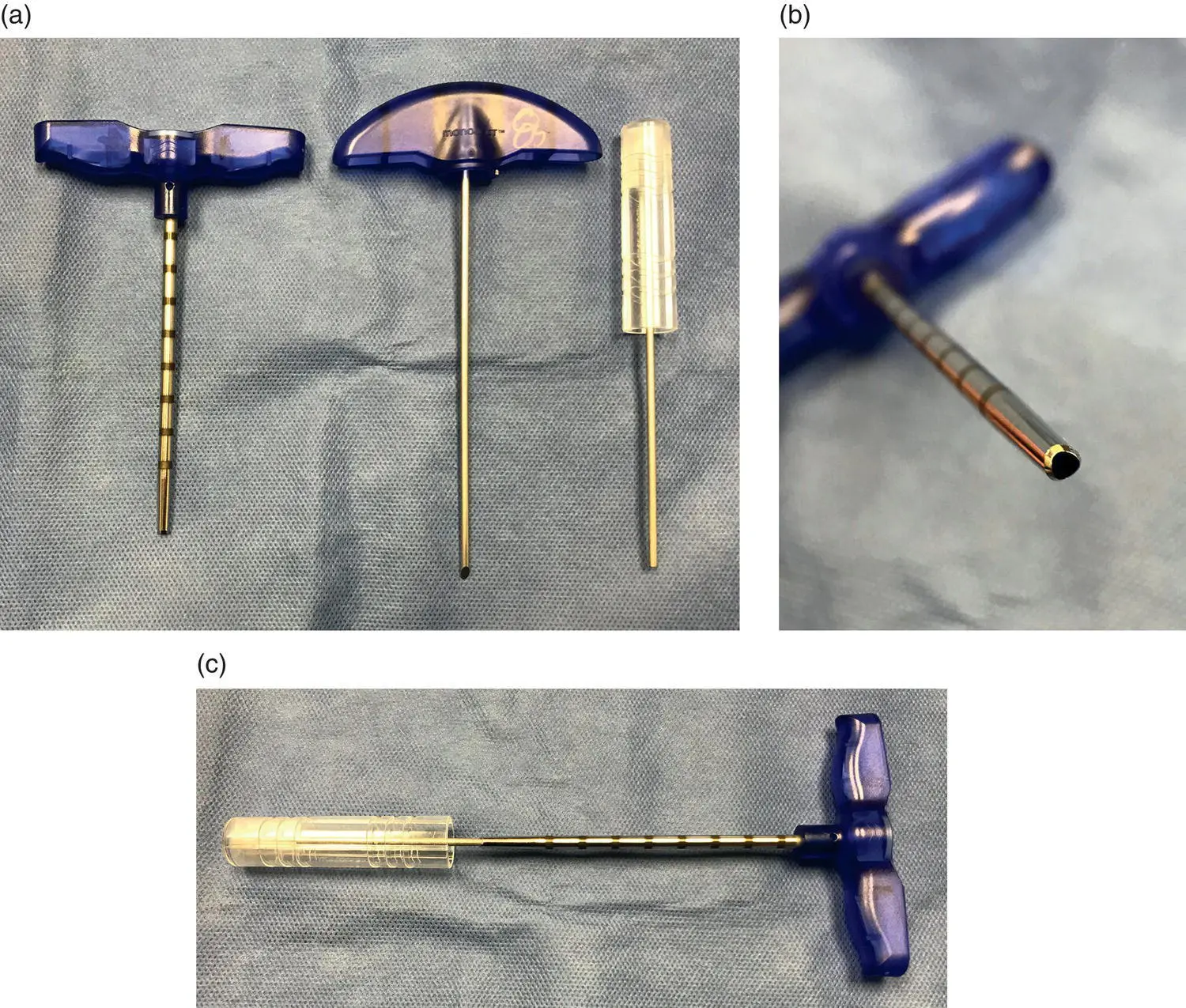
Figure 1.5 (a) Jamshidi needle (left) with the two stylets (middle and right). The stylet in the middle is used to approach the bone. The stylet to the right is used to remove the sample from the needle after being acquired. (b) The end of the needle is tapered, helping to keep the sample in the needle when the needle is removed from the bone. (c) To remove the sample from the needle, the stylet is introduced through the tip of the needle and the sample is pushed to exit the base at the handle. In some instances, there is too much resistance to push the sample out of the handle end, in which case the first stylet is used to push the sample out through the tip. It is not ideal because in theory the sample can suffer some damage going through the narrowed end, but sometimes it is necessary.
Endoscopic Biopsy
Esophagoscopy, gastroscopy, duodenoscopy, and colonoscopy are routinely performed in veterinary medicine as minimally invasive techniques to attain biopsies of the gastrointestinal tract. Biopsies attained during these procedures are generally smaller than what can be achieved with an open procedure; however, the biopsies are often diagnostic, and the morbidity associated with these procedures is reduced over open procedures (Magne 1995; Moore 2003).
Laparoscopy and thoracoscopy are still relatively underutilized modalities, but successful procurement of kidney, bladder, liver, spleen, adrenal gland, pancreas, stomach, intestine, and lung biopsies have been described by the use of these procedures (Rawlings et al. 2002; Lansdowne et al. 2005; Vaden 2005; Barnes et al. 2006). Case selection is essential when considering these minimally invasive alternatives, as cases that have excessively large tumors or other potential contraindications should undergo an open procedure.
Laparoscopy and thoracoscopy may have a role in the staging of veterinary patients as the use of these techniques increases. In cases where lymph node evaluation and biopsy would assist in predicting outcome or determining treatment, these procedures could be performed by minimally invasive techniques (Fagotti et al. 2007; Steffey et al. 2015; Lim et al. 2017).
Surgical Considerations for Curative‐Intent Surgery
Certain surgical technical principles will improve the chance of success and minimize the risk of local or distant seeding of tumor cells. The tumor should be draped off from the rest of the surgical field. Surgeons should attempt to not contact ulcerated or open areas of tumor with gloves or instruments. Sharp dissection is preferred over blunt dissection, when possible, as this will decrease the likelihood of leaving neoplastic cells within the patient and decrease the risk of straying from the preestablished margin. Tension on skin closures should be avoided whenever possible, especially in cases that have undergone radiotherapy. Proper knowledge of tension‐relieving techniques such as tension‐relieving sutures and flaps can assist in closure (Soderstrom and Gilson 1995; Aiken 2003); however, tension‐relieving skin incisions are contraindicated after removal of a neoplasm. If an indwelling drain is deemed necessary in a tumor resection site, the drain should be located in an area that can be resected during a subsequent surgery or in an area that will not compromise radiation therapy and can easily be included in the radiation field. Lastly, control of hemostasis and prevention of seroma or abscess development due to dead space is encouraged. Seromas or hematomas following an incomplete resection allow tumor cells to gain access to areas beyond the surgical field as these fluids may be widely dispersed throughout the subcutaneous space during movement.
To decrease the risk of recurrence after tumor resection, there are several techniques that the surgeon should practice. For tumors that have been previously biopsied or for which a drain has been placed, the biopsy tract and/or drain hole need to be removed en bloc with the tumor. Similarly, adhesions should be removed en bloc with the tumor, when possible. Leaving any of these can result in an increased risk of tumor recurrence. Additionally, when establishing a margin during surgical dissection, this margin must be maintained around the periphery of the tumor down to the deep margin. Straying from this may result in an incomplete resection. Similarly, the pseudocapsule present around a tumor should not be penetrated, as this pseudocapsule is constructed of a compressed layer of neoplastic cells (Soderstrom and Gilson 1995). Seeding of these cells will likely result in recurrence, and healing may be inhibited. Lastly, it is important that a new set of instruments, gloves, and possibly drapes be utilized for closure of a wound created by tumor removal or reconstruction of a wound. This principle applies to the removal of subsequent tumors on the same patient, as these items should not be transferred from one surgical site to another.
Defining and Evaluating Surgical Margins
The evaluation of surgical margins of an excised specimen is an essential component to appropriate care in a cancer patient. A surgical margin denotes a tissue plane established at the time of surgical excision, the tissue beyond which remains in the patient. Excised masses should be submitted in their entirety for evaluation of the completeness of excision. The surgeon should indicate the margins with ink or some other method prior to placing the specimen in formalin to aid the pathologist in identifying the actual surgical margin. Because the larger tumor specimen is trimmed by a technician to fit on a microscope slide, the pathologist may not be oriented as to what represents a surgical margin versus a sectioning “margin.” Tissue ink on the surgical margin allows there to be orientation throughout sectioning. The ink is present throughout the processing of the tumor specimen and is visible on the slide. If tumor cells are seen at the inked margin under the microscope, the surgical margin is by definition “dirty” or incomplete.
There is considerable confusion and controversy surrounding the issue of appropriate surgical margins and clinical decision‐making when histologically incomplete margins are obtained. Prior dogma has suggested that an overly generous margin is likely to be curative. In order to ensure a good oncological outcome, surgical oncologists have been trained to be as aggressive as possible. While it is well‐accepted that aggressive surgical margins tend to lead to better local control, this is not true in every case. Even extensive, complete surgical margins do not always lead to a cure. Local recurrence and/or metastasis may occur despite a histologically complete margin. Mounting evidence in the human sarcoma literature seems to suggest that a planned and executed “widest” surgical margin has not resulted in sufficient improvements in disease‐free intervals to justify the morbidity incurred with such resections. This opinion among human surgeons is confounded by the routine use of adjuvant radiation therapy in traditionally difficult‐to‐resect tumors such as extremity sarcomas. In veterinary medicine, adjuvant radiation therapy may not be available or affordable. As we know from experience and from the veterinary literature, not every patient with a histologically positive margin will experience recurrence. To confound things further, different malignancies and grades of malignancy (mast cell tumor vs. soft tissue sarcoma, low grade vs. high grade) may require specific and separate guidelines for margin planning.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Veterinary Surgical Oncology»
Представляем Вашему вниманию похожие книги на «Veterinary Surgical Oncology» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Veterinary Surgical Oncology» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.