Veterinary Surgical Oncology
Здесь есть возможность читать онлайн «Veterinary Surgical Oncology» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Veterinary Surgical Oncology
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Veterinary Surgical Oncology: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Veterinary Surgical Oncology»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
The new edition of the most comprehensive resource on surgical oncology, covering both basic and advanced surgical oncology procedures in small animals Veterinary Surgical Oncology
Veterinary Surgical Oncology
Veterinary Surgical Oncology, Second Edition
Veterinary Surgical Oncology — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Veterinary Surgical Oncology», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Incisional (Wedge) Biopsy
This technique is effective for masses in all locations and generates a larger sample for histopathologic evaluation as compared to the needle core biopsy. The location of the incision should be carefully planned, as the biopsy incision will need to be removed during the definitive treatment. Care should be taken to avoid dissection and prevent hematoma or seroma formation as these may potentially seed tumor cells into the adjacent subcutaneous space. Although the junction of normal and abnormal tissue is often mentioned as the ideal place to obtain a biopsy sample, one should take care to avoid entering uninvolved tissues. The most important principle to consider is to obtain a representative sample of the mass. It is also important to obtain a sample that is deep enough and contains the actual tumor, rather than just the fibrous capsule surrounding the mass. Incisional biopsy has a higher potential for complications such as bleeding, swelling, and infection due to the increase in incision size and dissection.
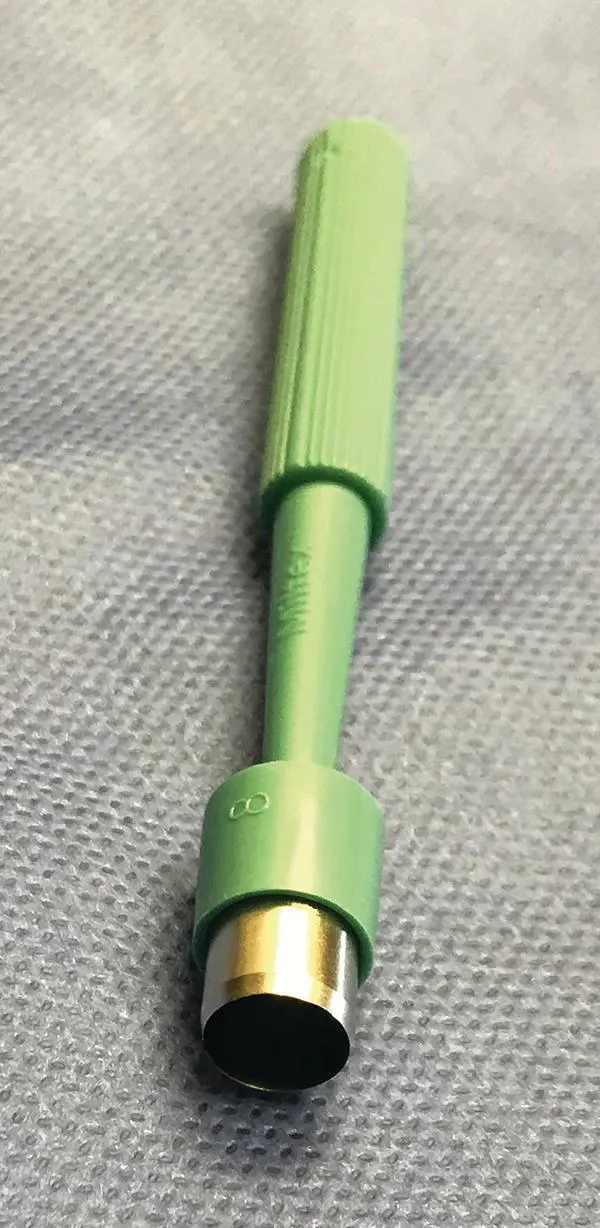
Figure 1.4 Punch biopsy instrument, 8 mm in diameter.
Instrumentation includes a scalpel blade, local anesthetic, Metzenbaum scissors, forceps, suture, and hemostats. A Gelpi retractor or similar self‐retaining retractor aids in visualization if the mass is covered by skin. If the skin is intact and moveable over the mass, a single incision is made in the skin. Once the tissue layer containing the tumor is exposed, two incisions made in a parallel direction are started superficially and then meet at a deep location to form a wedge. The wedge is then grasped with forceps and removed. If the deep margin of the wedge is still attached, the Metzenbaum scissors can be used to sever the biopsy sample free of the parent tumor. The wedge site is then closed with a suture.
Excisional Biopsy
The approach to an excisional biopsy is variable based on location, goal of surgery, and predetermined adjuvant therapy. An excisional biopsy has the advantage of being both a diagnostic technique as well as a treatment modality. A great deal of caution should be exercised in cases where the diagnosis is unclear. At a minimum, an FNA should be obtained to discern if a given mass is inflammatory or neoplastic and, if neoplastic, whether benign or malignant. This information is imperative in order to determine surgical dose.
There are cases where an excisional biopsy may be a reasonable option, if doubt or absence of knowledge of the tumor type remains after fine needle aspiration (e.g. nondiagnostic results from cytology), depending on the size and location of the tumor. In these instances, the surgeon must contemplate if an excisional biopsy will compromise the ability to enact a cure by wide excision. If it is deemed that an excisional biopsy can be performed while leaving this option, an excisional biopsy can be considered. For example, a 1 cm in diameter mass on the trunk of a large breed dog can be interrogated by excisional biopsy, whereas a 1 cm in diameter mass on the distal extremity of a dog should be interrogated by incisional biopsy (wedge or punch).
Once an excision is performed, the local anatomy is forever altered, tissue planes both deep and wide to the tumor are invaded, providing an opportunity for the tumor cells to extend and seed deeper and wider into tissues. For this reason, the best chance for complete excision is at the time of the first surgical excision. In order to perform a curative surgery, the surgeon must take the appropriate margin of tissue for the tumor type. In some cases (lipoma), this margin is minimal or even intralesional. In other cases (soft tissue sarcoma), the margin should be more extensive. Unless the tumor type is known at the time of excision, the surgeon may compromise the patient by doing too little or too much surgery.
Specific Biopsy Techniques
Bone Biopsy
The clinician performing the bone biopsy procedure should consider the eventual definitive treatment that is likely to be pursued for each case. The biopsy tract or incision needs to be in a location that can be removed during the definitive treatment. A reactive zone of bone exists in the periphery of most bone tumors, and samples taken from this region are more likely to result in an incorrect diagnosis (Wykes et al. 1985;, Liptak et al. 2004). The surgeon should target the anatomic center of the bony lesion. Two radiographic views of the involved bone should be available during the procedure as this will aid in optimal sampling. The majority of bone biopsies are performed utilizing either a Michele trephine or a Jamshidi needle (Wykes et al. 1985; Powers et al. 1988; Liptak et al. 2004). A trephine instrument provides a large sample and has been associated with 93.8% diagnostic accuracy (Wykes et al. 1985). The disadvantages of the trephine technique include increased likelihood of fracture as compared to other techniques, requirement of a surgical approach, and a more lengthy decalcification time prior to sectioning (Wykes et al. 1985; Ehrhart 1998).
Michele trephines are available in variable diameters. As a small surgical approach is required, a simple surgical pack is needed for the procedure. The biopsy site is clipped free of fur, and the patient is prepared with aseptic technique and draped. A 1–3 cm incision is made over the bony lesion, and the soft tissues are dissected from the surface of the tumor. The trephine is then seated into the tumor using a twisting motion. The trephine is advanced through the cis cortex. An effort should be made to not penetrate both the cis and trans cortex as fracture of the bone is more likely (Liptak et al. 2004). Once the trephine is within the medullary cavity, the trephine is rocked backed and forth to loosen the sample and then removed. A stylet is introduced into the trephine to push the sample out of the trephine onto a gauze square.
The Jamshidi needle technique is considered a less invasive means of obtaining a bone biopsy as compared to a Michele trephine. A small stab incision is necessary to introduce this device and fractures are unlikely. Although a more recent study suggests bone biopsies with a Jamshidi needle are only 82% accurate (Sabattini et al. 2017), an earlier study found that in approximately 92% of cases, a correct diagnosis of tumor versus nontumor is achieved when using a Jamshidi needle (Powers et al. 1988).
Instrumentation includes a #11 blade and a Jamshidi needle ( Figure 1.5). The surgical site is clipped free of fur, and the patient is prepared with aseptic technique and draped. A 1–2 mm stab incision is made over the bony lesion. The Jamshidi needle is introduced into the stab incision and pressed onto the bony lesion. The stylet is then removed from the needle, and the needle is twisted until the cis cortex is penetrated. The Jamshidi needle is rocked back and forth to loosen the sample and then removed. The stylet is reintroduced into the needle in the opposite direction of the initial location. As the stylet is moved through the Jamshidi needle, the biopsy will be ejected from the base of the Jamshidi needle.
For lesions that are large enough to be palpated, image guidance is not necessary. However, for small nonpalpable lesions, image guidance is recommended to document that the biopsy samples were indeed acquired from the lesion, preferably the center of the bone lesion. Fluoroscopy and radiography can be used and sometimes even CT‐guidance can be helpful.
Lymph Node Biopsy
Treatment and biopsy of lymph nodes in neoplastic disease remain controversial (Gilson 1995). It is demonstrated that lymph node size (Langenbach et al. 2001; Williams and Packer 2003) and needle aspirates are not great at detecting metastases (Ku et al. 2017; Fournier et al. 2018). Removing a lymph node or performing an incisional biopsy of a lymph node can aid in staging the patient and assist in the determination of prognosis or treatment options. The surgical oncologist should have a thorough knowledge of the anatomic location of the probable draining lymph node for a mass in a particular location. Alternatively, sentinel lymph node detection techniques such as lymphography and scintigraphy can be used (see Chapter 14). The excisional biopsy of superficial lymph nodes such as the mandibular, superficial cervical (prescapular), axillary, inguinal, or popliteal lymph nodes is described below. For removal of lymph nodes within the thorax or abdomen, an exploration of that body cavity is performed and the lymph nodes are removed by careful dissection and maintenance of hemostasis.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Veterinary Surgical Oncology»
Представляем Вашему вниманию похожие книги на «Veterinary Surgical Oncology» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Veterinary Surgical Oncology» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.