Veterinary Surgical Oncology
Здесь есть возможность читать онлайн «Veterinary Surgical Oncology» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Veterinary Surgical Oncology
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Veterinary Surgical Oncology: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Veterinary Surgical Oncology»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
The new edition of the most comprehensive resource on surgical oncology, covering both basic and advanced surgical oncology procedures in small animals Veterinary Surgical Oncology
Veterinary Surgical Oncology
Veterinary Surgical Oncology, Second Edition
Veterinary Surgical Oncology — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Veterinary Surgical Oncology», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Surgical Planning
The first decision in the surgical planning in removing a tumor is to determine the “surgical dose.” The surgical dose refers to how aggressive the excision is with respect to the edges of the tumor. The surgical dose has been divided into: intracapsular, marginal, wide, and radical ( Figure 1.1). An intracapsular excision is where the capsule of the organ where the tumor arises from (e.g. thyroid gland) or the pseudocapsule of the tumor (e.g. soft tissue sarcoma) is disrupted and the tumor is removed in pieces. A marginal excision is where the removal is done just outside or on the capsule or pseudocapsule. Oftentimes, the tumor is “shelled out.” A wide excision is when the tumor and its capsule are never entered and grossly normal tissue surrounds the specimen. This is often defined as 2–3 cm of normal tissue around the edges of the tumor and one fascial place beneath the cutaneous and subcutaneous tumors. The 2–3 cm of normal tissue is in situ and not histological. A radical excision is the removal of the entire compartment or structure where the tumor is arising from. An example of a radical excision is a limb amputation.
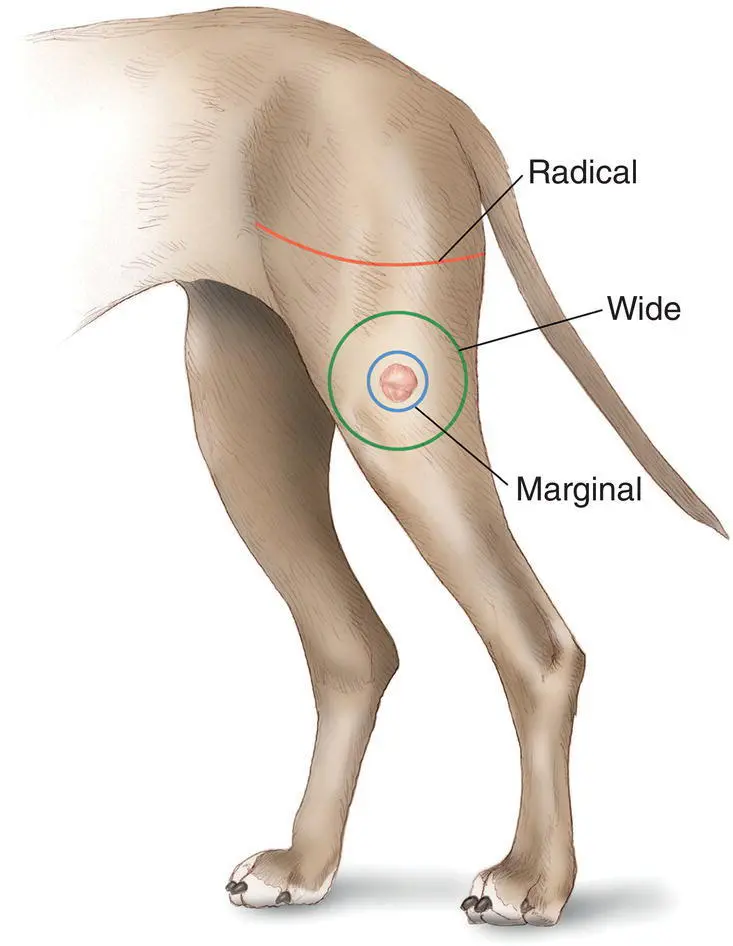
Figure 1.1 Diagram illustrating the different doses of surgery: marginal, wide, and radical being an amputation in this example. Intracapsular is not shown.
Source: Illustrated by Molly Borman.
When removing a tumor, there can be three different goals: curative, palliative, and cytoreductive. These goals will dictate the dose of surgery and several factors will guide which goal should be pursued. The first factor is tumor type. Because benign tumors are limited to their capsule and do not extend into the normal‐appearing tissues, a marginal excision is performed. Malignant tumors, however, have the ability to extend into the grossly normal‐looking tissue at the microscopic level ( Figure 1.2). Other factors need to be considered to determine the goal and consequently the dose of surgery. With (most) malignant tumors, when the goal is curative, a wide or radical excision is required. For a palliative or cytoreductive goal, a marginal excision is performed. An intracapsular excision is rarely indicated.
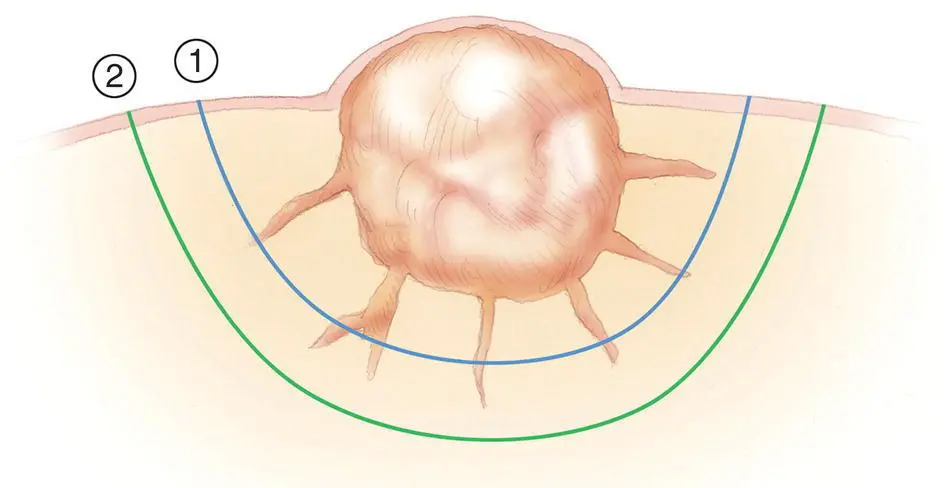
Figure 1.2 Diagram showing the extension of tumor into the grossly normal‐looking tissue. These extensions are most typically at the microscopic level. This is the reason to perform a wide excision (2), as opposed to a marginal excision (1), with the goal to achieve a complete excision.
Source: Illustrated by Molly Borman.
The additional factors to consider to determine the goal of the surgery are: tumor size and location, stage of the cancer, overall health of the patient, risk of the surgery, prognosis, and goals of the owners. Table 1.1provides examples of how these factors come into play, understanding there are always exceptions or nuances (see section on margins and palliative and cytoreductive surgery).
Because knowing the tumor type is essential in most instances, methods to get a diagnosis are a fine needle aspirate (FNA) or biopsy.
Fine Needle Aspirate
Fine needle aspiration is often the most minimally invasive technique for obtaining critical information about a newly identified mass prior to surgery. The accuracy of a FNA is dependent on many factors including the tumor type, location, and amount of inflammation. Overall sensitivity and specificity of cytology have been reported to be 89% and 100%, respectively (Eich et al. 2000; Cohen et al. 2003). Imaging tools such as ultrasound and fluoroscopy can increase the chance of obtaining a diagnostic sample.
In most patients, an FNA of cutaneous or subcutaneous lesions can be obtained with no sedation and a minimal amount of discomfort. Fine needle aspiration has been compared to histopathologic samples in several studies. In one study of the correlation between cytology generated from fine needle aspiration and histopathology in cutaneous and subcutaneous masses, the diagnosis was in agreement in close to 91% of cases (Ghisleni et al. 2006). Cytology was 89% sensitive and 98% specific for diagnosing neoplasia, and these numbers varied slightly based on tumor type (Ghisleni et al. 2006). For example, both the sensitivity and specificity were 100% for mast cell tumors (Ghisleni et al. 2006). In one study looking at the accuracy of cytology of lymph nodes in dogs and cats, cytology had a sensitivity of 67%, specificity of 92%, and accuracy of 77% for a diagnosis of neoplasia (Ku et al. 2017). In that study, 31% of metastatic lymph nodes secondary to a mast cell tumor were falsely negative (Ku et al. 2017). In another study evaluating the value of cytology of lymph nodes to detect metastasis of solid tumors, the sensitivity of needle aspirates of the lymph node was 67% for sarcomas, 100% for carcinomas, 63% for melanomas, 75% for mast cell tumors, and 100% for other round cell tumors. The specificity varied between 83 and 96%; also, 20% of nondiagnostic samples were metastatic (Fournier et al. 2018).
Table 1.1 Factors affecting the goal of surgery and consequently the dose of surgery
| Tumor type | stage | Size | location | Owner’s goals | prognosis | Overall health of patient | Goal of surgery | Dose of surgery |
|---|---|---|---|---|---|---|---|---|
| Benign | Marginal | |||||||
| Malignant | Metastasis present | Palliative | Marginal | |||||
| No metastasis | Small | Trunk | Good to excellent | Good | Curative | Wide | ||
| Significant | Limb | Owners accept amputation | Good to excellent for function | Good | Curative | Radical | ||
| Significant | Limb | Owners refuse amputation but accept surgeries with higher morbidity and risks | Good for local control and long term survival | Good | Curative | Wide (with reconstructive surgery) | ||
| Significant | Limb | Owners refuse amputation or surgeries with higher morbidity and risks | Good with adjuvant therapy | Good | Cytoreductive | Marginal | ||
| Significant co‐morbidities | Palliative | Marginal |
The goal of fine needle aspiration is to differentiate between an inflammatory or neoplastic process and, if neoplastic, whether the tumor is benign or malignant. In some cases, the specific tumor type can be determined (e.g. mast cell tumor). In other cases, the class of tumor may be identified (e.g. sarcoma), but the specific diagnosis requires histopathology (e.g. chondrosarcoma versus osteosarcoma). The overall purpose of obtaining the FNA is to guide the staging diagnostics (where to look for metastasis or paraneoplastic diseases) and surgical dose. For example, an FNA of a mass showing normal adipocytes would indicate the mass is not inflammatory, rather it is a neoplastic process and it is benign (lipoma). Based on the knowledge of the biologic behavior of this tumor, no other staging tests would be performed and minimal surgical dose would be prescribed (marginal resection). Alternatively, if the FNA of a mass indicated carcinoma cells, more advanced staging (three‐view thoracic radiographs, abdominal ultrasound and/or thoracic and abdominal CT, lymph node aspirates) would be indicated and a larger surgical dose would be prescribed.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Veterinary Surgical Oncology»
Представляем Вашему вниманию похожие книги на «Veterinary Surgical Oncology» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Veterinary Surgical Oncology» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.