Irene Roberts - Neonatal Haematology
Здесь есть возможность читать онлайн «Irene Roberts - Neonatal Haematology» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Neonatal Haematology
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Neonatal Haematology: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Neonatal Haematology»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Neonatal Haematology — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Neonatal Haematology», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
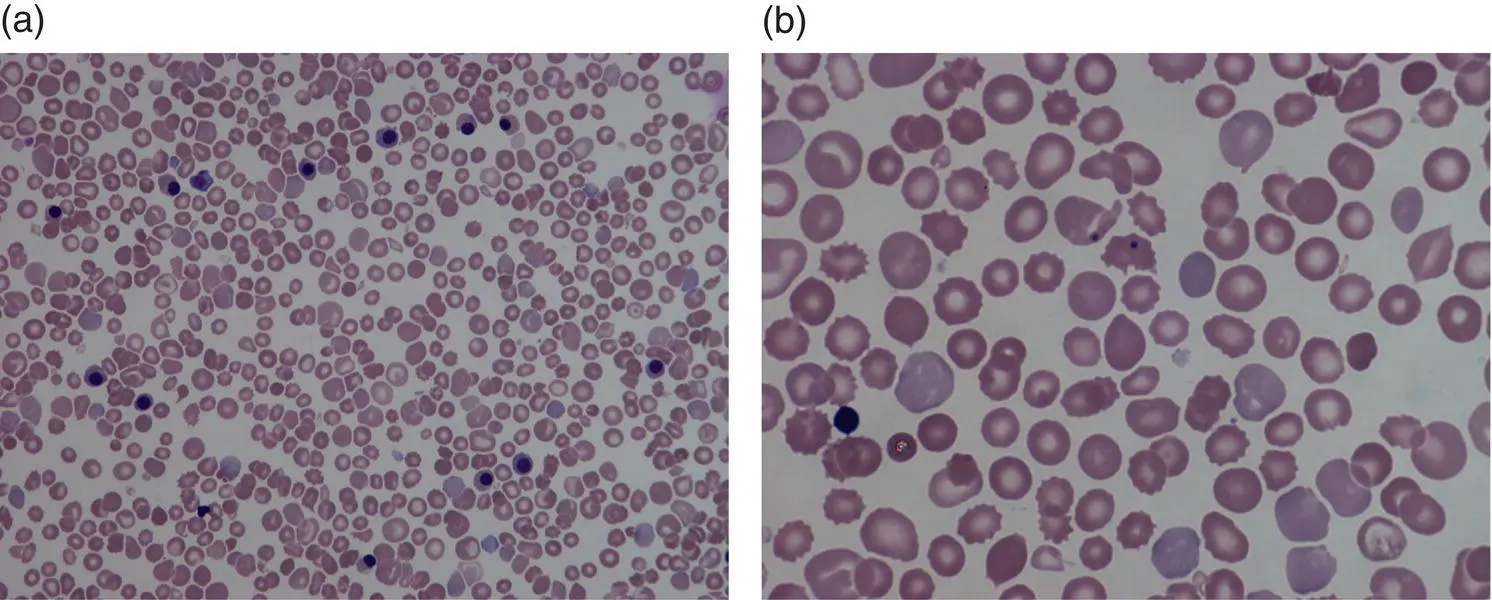
Fig. 1.10 Blood film showing features of hyposplenism resulting from intrauterine growth restriction: (a) low power showing anisocytosis, poikilocytosis, target cells and some fragments (MGG, ×40); (b) high power, two Howell–Jolly bodies are apparent (MGG, ×100).
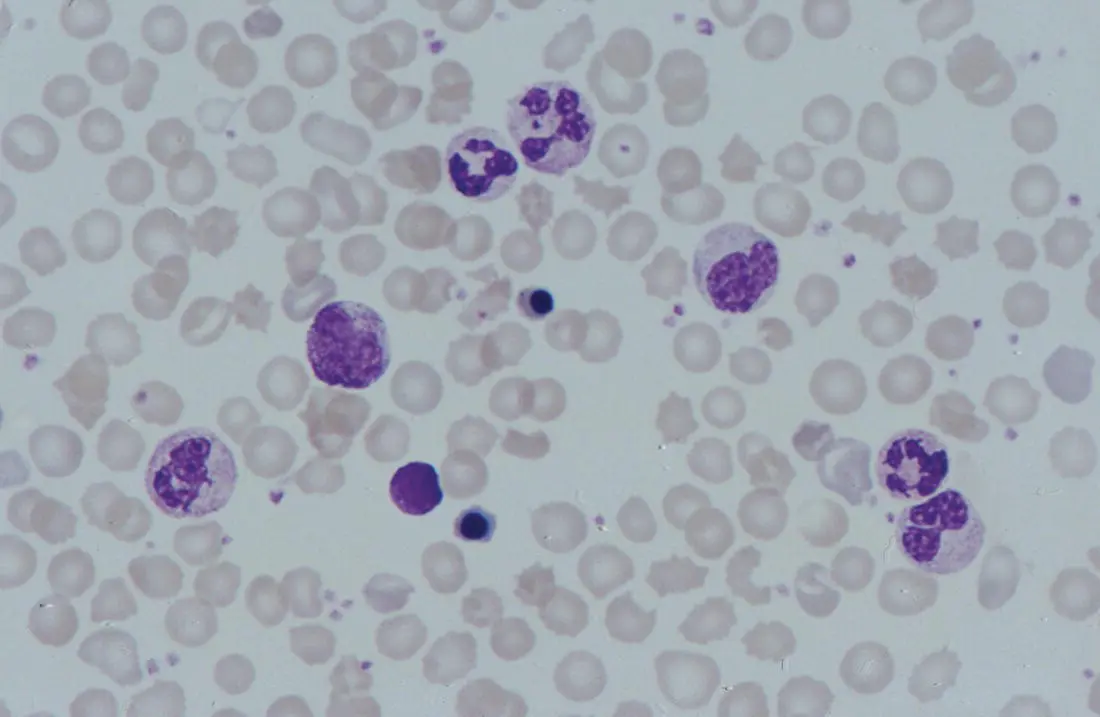
Fig. 1.11 Blood film from a preterm neonate (born at 25 weeks’ gestation) on the day of birth showing a leucoerythroblastic picture with NRBC, a myelocyte and promyelocyte as well as toxic granulation of the neutrophils and red cell morphology typical of an extremely preterm neonate. This appearance is typical of perinatal hypoxia. MGG, ×100.
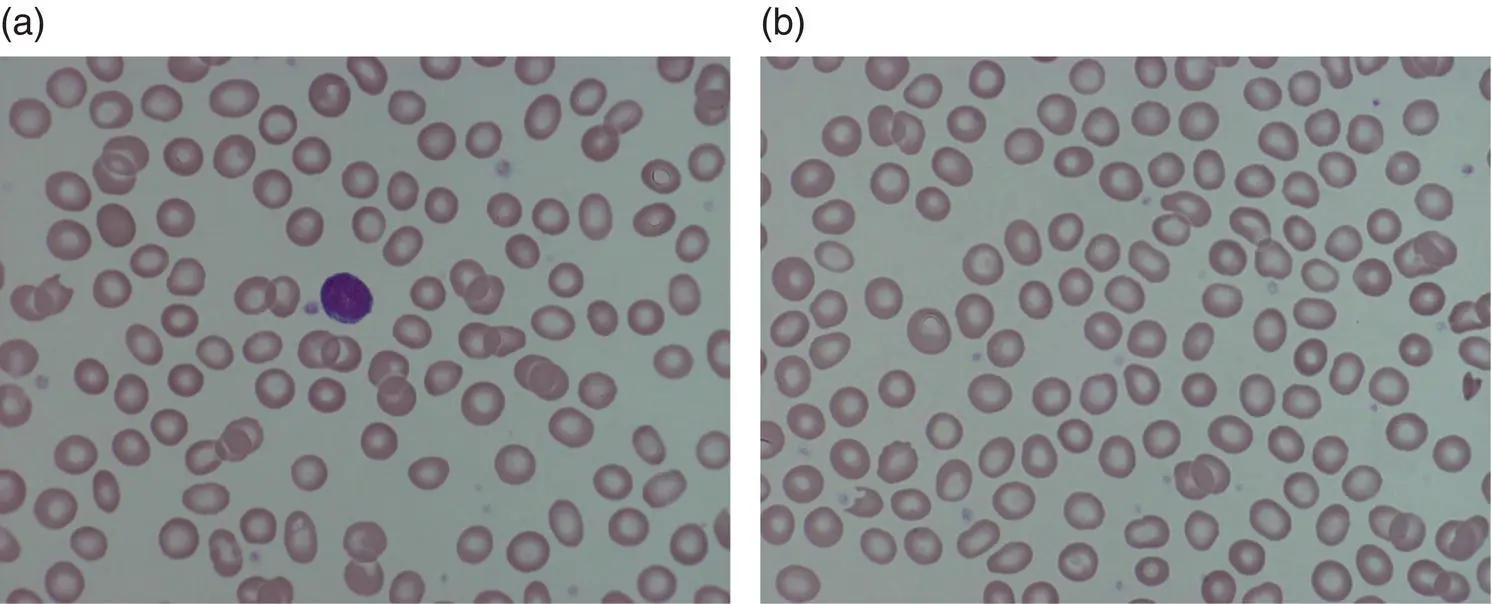
Fig. 1.12 Impact of postnatal age on red cell morphology; blood films from: (a) healthy term baby; (b) neonate at a postnatal age of 4 weeks. MGG, ×100.
The presence of a small proportion (typically <5%) of spherocytes and target cells in the first few days of life is normal, particularly in preterm babies, possibly reflecting a degree of functional hyposplenism in the neonate. Consistent with this, these features are more marked in neonates with IUGR, when they are usually accompanied by the presence of Howell–Jolly bodies 34(see Fig. 1.10). The presence of schistocytes in neonatal blood films may cause confusion. When they are present in large numbers in the first few days of life they may be an indicator of a microangiopathic process, as seen in disseminated intravascular coagulation (DIC), thrombotic thrombocytopenic purpura or Kasabach–Merritt syndrome. On the other hand, the presence of large numbers of schistocytes (10–20%) is very common in well babies for several months after the first few weeks of life (personal observation) and may simply reflect residual damaged fetal erythrocytes yet to be cleared from the circulation (see Fig. 1.12). Care should therefore be taken not to overestimate the significance of schistocytes in well babies with otherwise normal blood counts or mild physiological anaemia.
Blood volume
The normal blood volume at birth varies with gestational age and the timing of clamping of the umbilical cord. 79In healthy term infants, the average blood volume is 80 ml/kg (range 50–100 ml/kg); however, this can be increased by up to 25% by late clamping of the cord. 79Estimates of the blood volume in preterm infants show a slightly higher range of 85–106 ml/kg, largely due to an increase in plasma volume. 80–82
Folic acid and vitamin B 12
In term and preterm babies of normally nourished mothers, stores of folic acid and vitamin B 12are adequate at birth and are maintained after birth in term neonates. 83However, infants that are breastfed and born to mothers who are vitamin B 12deficient, either due to vitamin B 12malabsorption or because of a strict vegetarian diet, are at high risk of developing severe vitamin B 12deficiency at 4–8 months of life. The prevalence of vitamin B 12deficiency at birth varies in different countries from less than 1 in 100 000 in the USA to 1 in 3000–5000 in European countries where neonatal screening studies have been performed. 84–87Although these infants are asymptomatic in the neonatal period, they develop progressive anaemia and neurological problems over the following months. 88Although the anaemia is rapidly reversible with intramuscular vitamin B 12, persistent neurological impairment has been reported, 89leading some to recommend neonatal screening for presymptomatic identification of vitamin B 12deficiency. 90In preterm infants, folic acid reserves are lower at birth and are depleted more quickly than in term neonates, causing deficiency after 2–4 months if the recommended daily intakes are not maintained. The recommended daily intake for folic acid in preterm neonates is 25–100 μg/kg. 91As preterm formula milks and breast milk fortifiers provide sufficient folic acid to prevent folate deficiency in preterm infants, 92further supplementation is not required unless there is chronic haemolysis.
Leucocytes in the fetus and newborn
The leucocytes that form the human blood and immune system in the developing fetus start to appear in the peripheral blood during the first trimester. 93Monocytes and lymphocytes appear in fetal blood by 8 weeks post‐conception, although initially in very low numbers. This is followed by the appearance of neutrophils and eosinophils from around 14–16 weeks post‐conception, once haemopoiesis begins to be established in the bone marrow, 9,16increasing by the end of the third trimester to the lower end of the values reported for leucocyte counts in term neonates. Blast cells are a normal feature in fetal blood, particularly in the second trimester, but are not usually greater than 10%. 94
Apart from alterations in the numbers of white blood cells in response to infection, leucocyte disorders are not common in neonates. Nevertheless, some diagnostic dilemmas do present in the neonatal period, particularly when there is neutropenia or a rare disorder such as congenital leukaemia is suspected. Careful evaluation of leucocyte morphology can not only help to make an early diagnosis of bacterial infection but can also suggest the type of bacterial infection and provide rapid clues to the presence of congenital viral infection or a rare genetic or metabolic disorder (see Chapter 3). In addition, automated leucocyte differential counts are often inaccurate in neonatal samples, particularly in very preterm neonates, so that validation from a blood film is important.
In contrast to the gestation‐related differences in red cell morphology, leucocyte morphology (neutrophils, monocytes, eosinophils, basophils and lymphocytes) is the same in healthy neonates of any gestation as in adults.
Leucocyte production and function in the fetus and neonate
All of the same types of normal leucocyte found in older children can be seen in peripheral blood films of term and preterm neonates ( Fig. 1.13), although their frequencies vary from those in older children and also vary both with gestational age and with postnatal age (see Table 1.2). Blast cells are the only cells commonly seen in neonatal blood films that are not usual in blood films from healthy older children or adults ( Fig. 1.14).
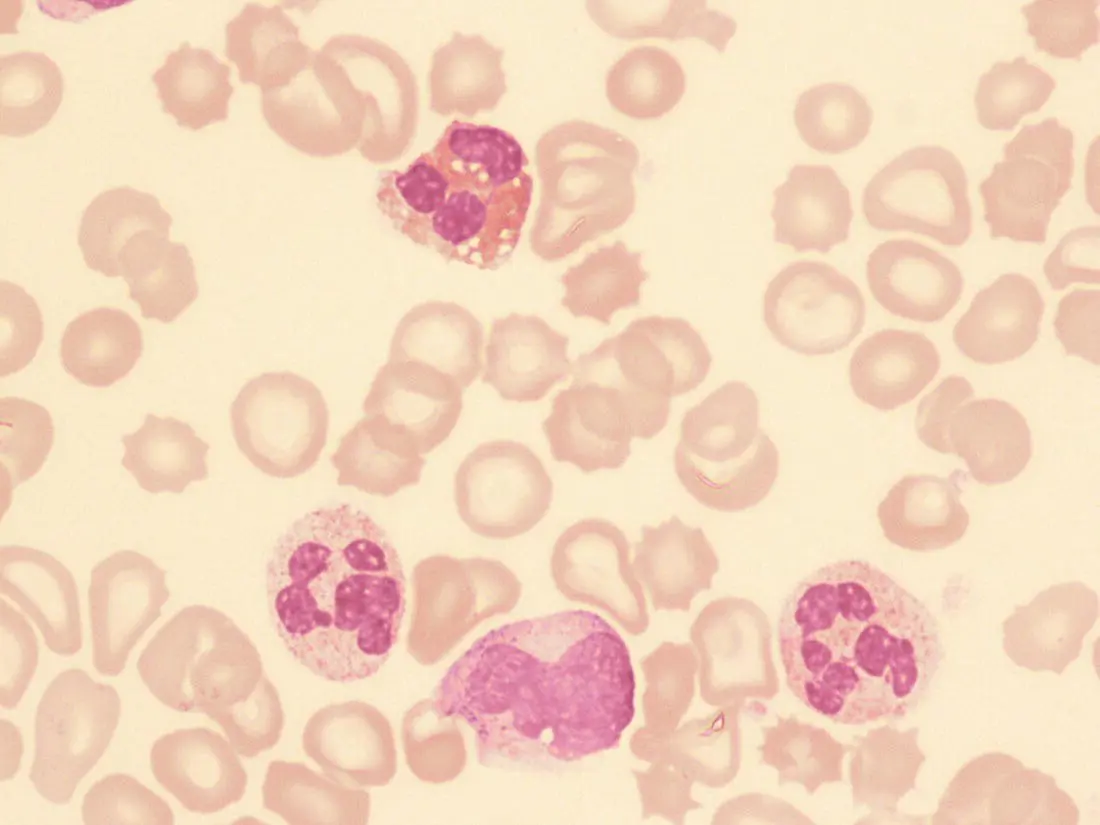
Fig. 1.13 Blood film of a preterm neonate showing normal white cells – two neutrophils, an eosinophil and a monocyte. MGG, ×100.
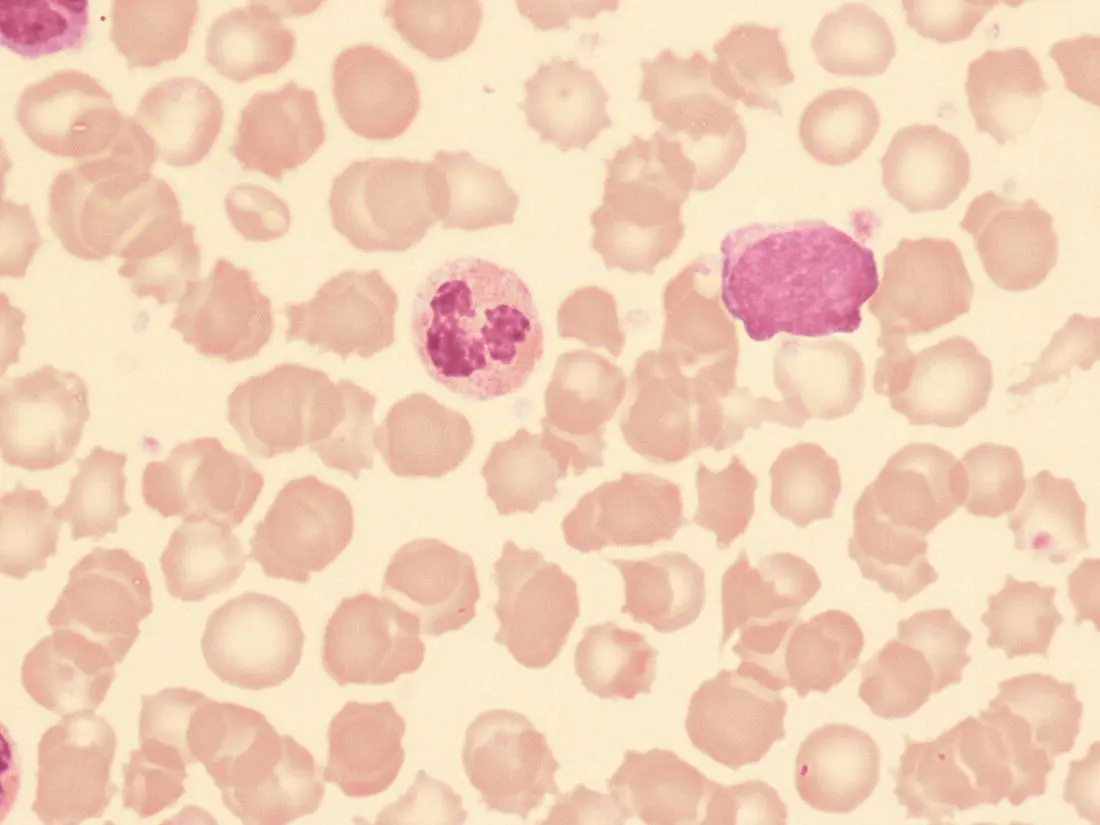
Fig. 1.14 Blood film of a healthy preterm neonate born at 25 weeks’ gestation showing a neutrophil and a blast cell. MGG, ×100.
There is increasing recognition that leucocyte function in the fetus and newborn differs from that in adults 95and that this is almost certain to contribute to the increased susceptibility to infection in neonates, particularly in those that are extremely preterm. 96As the adaptive immune system only properly develops with antigen exposure after birth, neonates are specifically dependent on the innate immune system as a first line of defence against bacterial and fungal pathogens in particular. 97Remarkably, all of the cellular components of the innate immune system are established in the human fetus over a small number of weeks late in the first trimester and early second trimester of fetal life. 16
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Neonatal Haematology»
Представляем Вашему вниманию похожие книги на «Neonatal Haematology» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.


Обсуждение, отзывы о книге «Neonatal Haematology» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.