Gastrointestinal Surgical Techniques in Small Animals
Здесь есть возможность читать онлайн «Gastrointestinal Surgical Techniques in Small Animals» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Gastrointestinal Surgical Techniques in Small Animals
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Gastrointestinal Surgical Techniques in Small Animals: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Gastrointestinal Surgical Techniques in Small Animals»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Describes techniques for canine and feline gastrointestinal surgery in detail Presents the state of the art for GI surgery in dogs and cats Includes access to a companion website with video clips demonstrating techniques
is an essential resource for small animal surgeons and veterinary residents.
Gastrointestinal Surgical Techniques in Small Animals — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Gastrointestinal Surgical Techniques in Small Animals», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Eric Monnet
Department of Clinical Sciences, College of Veterinary Medicine and Biomedical Sciences, Colorado State University, Fort Collins, CO, USA
5.1 Indications
Drainage of the peritoneal space has been mostly performed for the treatment of peritonitis (Salisbury and Hosgood 1989; Hosgood 1990; Hosgood et al. 1991; Ludwig et al. 1997; Staatz et al. 2002; Buote and Havig 2012; Adams et al. 2014). Septic peritonitis and chemical peritonitis are the two most common conditions that are treated with some form of drainage. The main goal of the drainage is to decrease the bacterial load and/or to reduce the amount of chemical present in the pleural space.
Drainage is mostly indicated for generalized septic peritonitis. Drainage is also indicated if the cause of the peritonitis could not be totally controlled at the time of surgery (pancreatitis). Drainage is also indicated for a septic peritonitis associated with severe contamination with foreign materials (rupture of colon). The risk versus benefit of drainage has not been evaluated in a prospective trial to demonstrate the true benefit of drainage. “Drains provide a false sense of security and re‐assurance; we have all seen the moribund post‐operative patient with an abdomen crying to be reexplored while his surgeon strongly denies any possibility of intraperitoneal catastrophe because the tiny drains he inserted in each abdominal quadrant are ‘dry' and nonproductive. We cannot produce high‐level evidence to support our aversion to drains, but the generations of surgeons who used drains for many years also never succeeded in proving their advantage” (Schein 2002).
Open drainage has been historically used mostly during the treatment of generalized septic peritonitis with either presence of lot of foreign materials in the pleural space or bile. Bile salts are very caustic and potentiate the virulence of bacteria. Open drainage of the peritoneal cavity is rarely recommended in human medicine for the treatment of peritonitis (Schein 2002).
Drainage of the peritoneal space should also reduce the risk of compartment syndrome resulting from the accumulation of abdominal effusion in the close space of the abdominal cavity. It might be the major benefit of the drainage of the peritoneal space (Schein et al. 1995; Schein 2002).
Drainage of a uroabdomen due to a ruptured urethra or bladder is an important component of the stabilization for the patient before abdominal surgery. Drainage of the urine present in the abdominal cavity is an important component of the treatment of hyperkalemia present with a uroabdomen. After placement of a percutaneous drain diuresis can be started to help lower the potassium level.
5.2 Techniques
Drainage of the peritoneal cavity can be achieved with either a closed suction drain, a negative pressure drainage system, or an open abdomen (Salisbury and Hosgood 1989; Hosgood 1990; Hosgood et al. 1991; Ludwig et al. 1997; Staatz et al. 2002; Buote and Havig 2012; Adams et al. 2014). Drains can be placed percutaneously with a local block or surgically during a laparotomy.
5.2.1 Percutaneous Placement of an Abdominal Drain
Drains that are placed percutaneously are usually temporary because they are getting wrapped in the omentum within 12–24 hours. Those drains should only be used for draining a uroabdomen to diurese the patient and help control hyperkalemia to be able to safely induce general anesthesia. Different drains have been used.

Figure 5.1
5.2.1.1 Passive Drain
A simple red rubber feeding tube can be used ( Figure 5.1). The red rubber feeding tube can be wrapped in a fenestrated Penrose drain to protect the red rubber feeding tube from the omentum.
The patient is placed in right lateral recumbency. After surgically preparing the left caudal abdominal wall, a local block with bupivacaine is performed in the skin and the abdominal wall where the drain is going to be inserted. A bolus of fentanyl can be given to the patient also. The puncture in the abdominal wall is 2–3 cm cranial to the skin incision. A small skin incision is performed with a #15 blade where the local block was performed. A 2–3 cm subcutaneous tunnel is created with a curved Carmalt forceps in a cranial direction toward the local block in the abdominal wall. The tip of the red rubber feeding tube is then grabbed by the curved Carmalt and advanced in the tunnel. The abdominal wall is then punctured with the Carmalt and the red rubber feeding tube. The tube is then advanced in the abdominal cavity.
The red rubber feeding tube is then secured to the skin with a Chinese finger trap with 2‐0 nylon. The tube is then connected to a passive collection system.
If a fenestrated Penrose drain is placed around the red rubber feeding tube it is inserted in a similar fashion than the simple red rubber feeding tube.
5.2.1.2 Closed Suction Drain
The patient is prepared as described above for the placement of a passive drain.
Usually a Seldinger technique is used to place a closed suction drain percutaneously. An 18G catheter is tunneled under the skin into the abdominal cavity. A wire is then advanced in the catheter into the abdominal cavity. The 18G catheter is then removed and the closed suction drain is advanced over the wire into the abdominal cavity.
The drain is secured to the skin with a Chinese finger trap with 2‐0 Nylon. The drain is then connected to a suction device and a reservoir. The device generates a negative pressure close to 10 mmHg. Usually the reservoir can be 100–400 ml depending on the size of the animal and the amount of effusion that is expected to be produced.
5.2.2 Surgical Placement of a Closed Suction Drain
According to the dynamic of fluids in the abdominal cavity, abdominal effusion moves from the caudal to cranial toward the diaphragm (Hosgood et al. 1989). Therefore drains need to be placed in the cranial part of the abdominal cavity between the liver lobes and the diaphragm. In this position the drain should be more efficient for collecting in the abdominal cavity and also it should keep the drain away from the omentum.
A Jackson–Pratt system, commonly made with a flat silicon drain, is placed in the abdominal cavity as described above ( Figure 5.2). The flat silicon drain comes in different diameters. The tube is tunneled throughout the abdominal wall and the skin with a sharp trocar. A trocar is used to create a tight seal of the abdominal wall, subcutaneous tissue, and skin around the tube. Usually the exit point is in the left or right caudal abdomen.
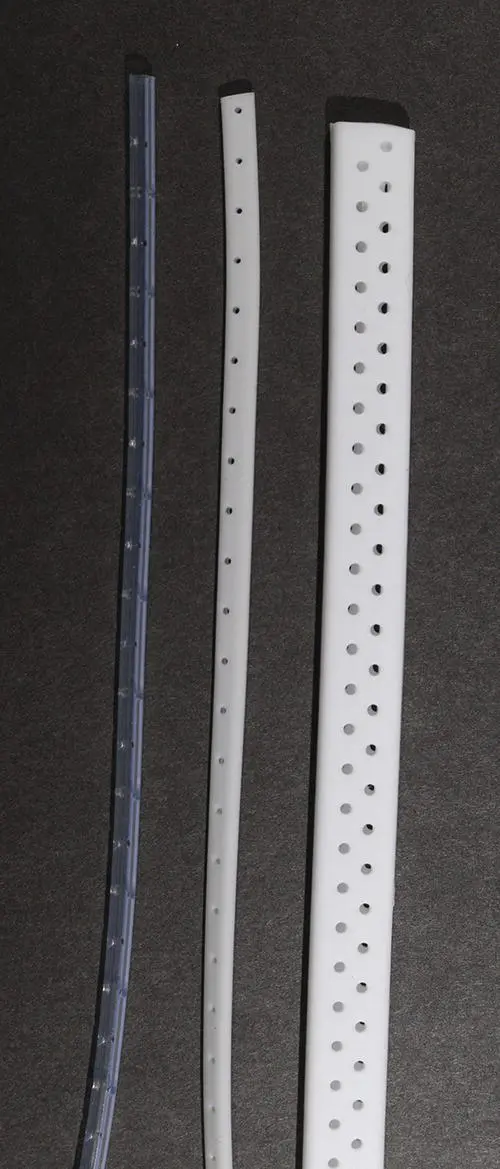
Figure 5.2
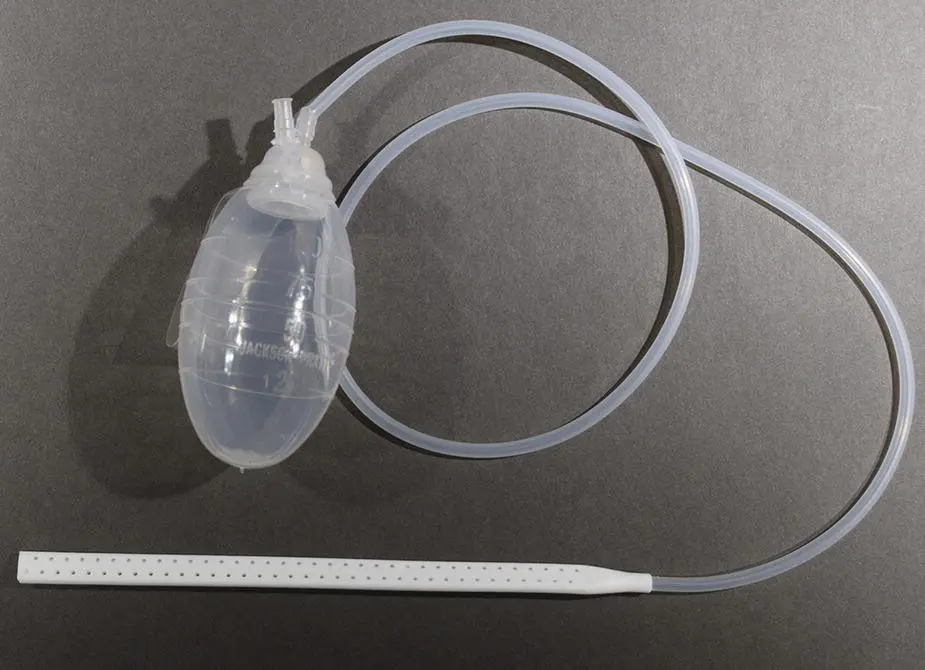
Figure 5.3
A Chinese finger trap is used to secure the drain to the skin. The drain and the reservoir have to be well protected to prevent accidental removal of the drain by the patient. A suction device with a reservoir is connected to the drain ( Figure 5.3). The device generates a negative pressure close to 10 mmHg. Usually the reservoir can be 100–400 ml, depending on the size of the animal and the amount of effusion that is expected to be produced. The reservoir has to be emptied as needed to maintain constant negative pressure in the abdominal cavity.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Gastrointestinal Surgical Techniques in Small Animals»
Представляем Вашему вниманию похожие книги на «Gastrointestinal Surgical Techniques in Small Animals» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.




Обсуждение, отзывы о книге «Gastrointestinal Surgical Techniques in Small Animals» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.