Gastrointestinal Surgical Techniques in Small Animals
Здесь есть возможность читать онлайн «Gastrointestinal Surgical Techniques in Small Animals» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Gastrointestinal Surgical Techniques in Small Animals
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Gastrointestinal Surgical Techniques in Small Animals: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Gastrointestinal Surgical Techniques in Small Animals»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Describes techniques for canine and feline gastrointestinal surgery in detail Presents the state of the art for GI surgery in dogs and cats Includes access to a companion website with video clips demonstrating techniques
is an essential resource for small animal surgeons and veterinary residents.
Gastrointestinal Surgical Techniques in Small Animals — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Gastrointestinal Surgical Techniques in Small Animals», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
4.3.3.2.2 Laparotomy
Gastrostomy tubes are frequently placed during a laparotomy. A purse‐string suture with 3‐0 monofilament absorbable suture is placed in the wall of the body of the stomach close to the junction with the fundus between the lesser and the greater curvature ( Figure 4.7a–f).
A #11 blade is then used to penetrate the abdominal wall from the skin surface. The blade is introduced caudal to the last rib lateral to the rectus abdominalis muscle. A large size forceps grabs the blade in the abdominal cavity. The blade is withdrawn from the abdominal wall with the forceps. The forceps then grabs the feeding tube and pulls it inside the abdominal cavity. A puncture is made in the center of the purse‐string in the wall of the stomach. The gastrostomy tube is then introduced in the lumen of the stomach and the purse‐string is tightened. If a Foley catheter has been used, the balloon is inflated with 5 ml of saline. Four pexy sutures are placed between the wall of the stomach and the transverse abdominalis muscle around the gastrostomy tube. A 3‐0 monofilament absorbable suture is used for the pexy sutures. A Chinese finger‐trap suture with 2‐0 nylon is placed on the skin to secure the tube.
The laparotomy is closed in a routine fashion.
4.3.4 Tips
The utilization of the #11 blade and the forceps to go through the abdominal wall minimizes the size of the incision made in the abdominal wall for the placement of the gastrostomy tube. It minimizes the risk of peristomal inflammation.
4.3.5 Utilization
Gastrostomy tubes are not used in the first 24 hours after placement to allow a seal to form between the stomach wall and the abdominal wall. Feedings are then conducted four times a day with a blenderized diet. The total daily caloric requirements are calculated and divided in four feedings. The amount of food is delivered over 5–10 minutes. The tube should be flushed with water after each feeding to prevent obstruction of the tube.
4.3.6 Complications
Gastroesophageal reflux and vomiting can occur if the gruel is delivered too fast or cold. Increasing the frequency of the feeding and reducing the volume of each feeding might also help reduce the risk of vomiting. Peristomal inflammation can happen if leakage occurs around the tube.
Gastrostomy tubes can be dislodged accidentally or pulled by the dog. Premature removal of the tube may result in leakage and peritonitis. If the tube has been pulled accidentally it is usually possible to replace it immediately with heavy sedation. A new Foley catheter can be introduced into the stoma. A radiograph with water‐soluble iodine is used to confirm placement of the new tube in the stomach. Obstruction of the tube can occur. It is important to regularly flush the tube with saline. If the tube cannot be cleared the tube will need to be replaced.
4.4 Jejunostomy Tube
4.4.1 Indications
Jejunostomy tubes are indicated when feeding in the stomach is not possible. It is used to bypass a diseased upper gastrointestinal tract, resulting in chronic vomiting. It is also indicated in surgery to bypass an enterotomy or enterectomy. Jejunostomy tubes are often placed during the surgical treatment of peritonitis to be able to provide nutrients to a hyper‐metabolic patient without increasing of gastroesophageal reflux and aspiration pneumonia (Marks 1998; Daye et al. 1999; Heuter 2004; Hewitt et al. 2004).
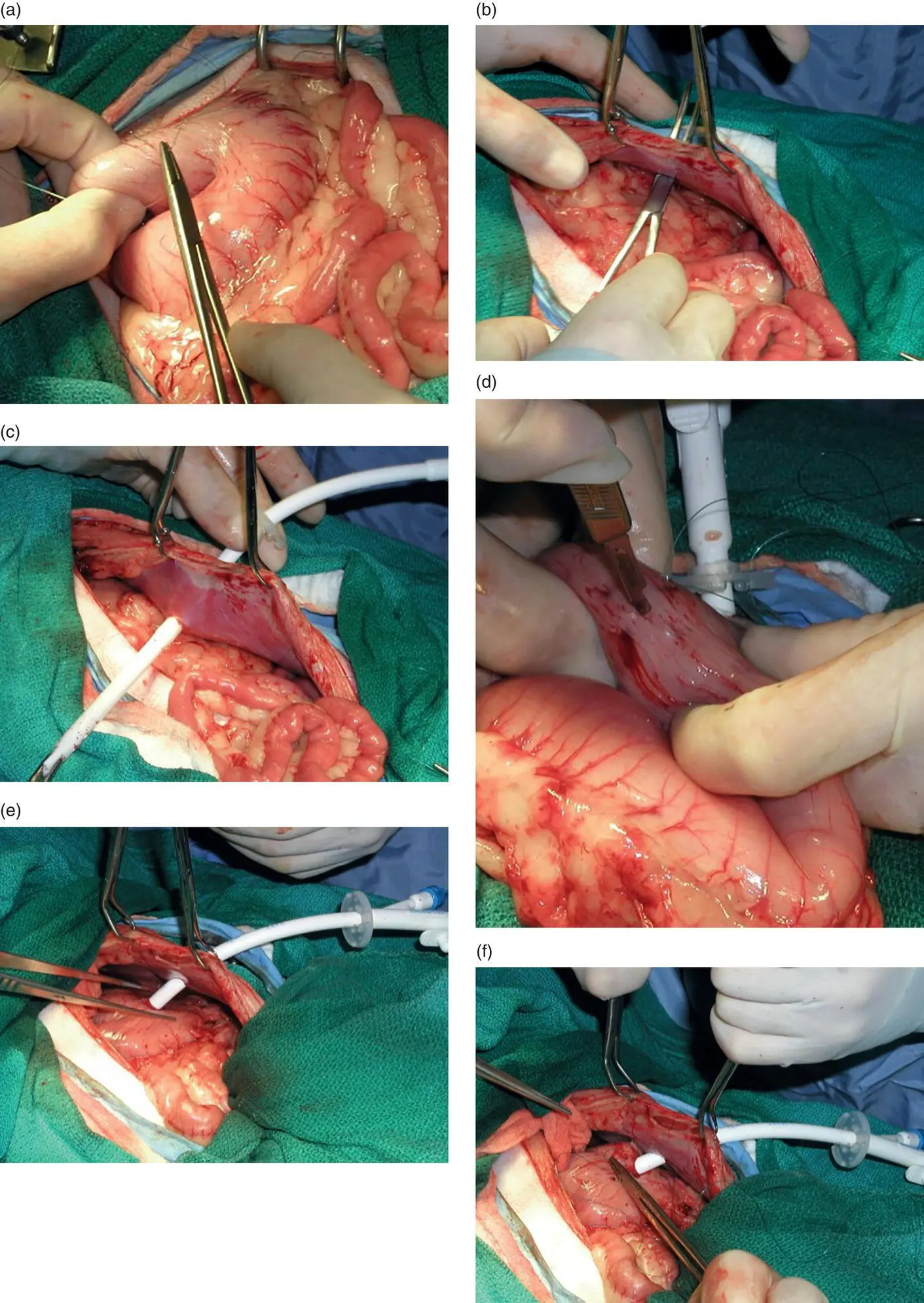
Figure 4.7
4.4.2 Materials and Equipment
A small long bore feeding is used for a jejunostomy tube. Usually tube from 5 to 9 Fr are used ( Figure 4.8). The tubes are 50–89 cm long.
General anesthesia is required for the placement of a jejunostomy tube.
4.4.3 Technique
4.4.3.1 Laparoscopically Assisted
Three separate cannulas are used. One cannula is placed where the jejunostomy tube is placed in the right side of the abdominal cavity ( Figure 4.9). A single‐access port can also be used and it is inserted in the middle of the right side of the abdominal cavity. The port is placed lateral to the rectus abdominalis muscle.
After insufflation of the abdominal cavity a 5 mm rigid endoscope and two 5 mm grasping forceps are used to visualize and manipulate the loop of jejunum. After identifying the most proximal loop of jejunum it is brought against the abdominal wall and the single‐access port is removed ( Figure 4.9a). The oral and aboral orientation of the loop of jejunum should be identified. A stay suture is placed in the wall of the jejunum. A 4‐0 monofilament absorbable suture is then used to place a purse‐string suture in the wall of the jejunum ( Figure 4.9b). A #11 blade is used to puncture the center of the purse‐string suture. The jejunostomy tube is then introduced in the lumen of the jejunum in the aboral direction ( Figure 4.9c). Usually 15–20 cm of the tube is placed in the jejunum. The purse‐string suture is tightened around the tube. Four pexy sutures are placed between the wall of the jejunum and the transverse abdominalis muscle ( Figure 4.9d and e). A 4‐0 monofilament absorbable suture is used for the pexy. The subcutaneous tissue and skin are closed in a routine fashion around the tube ( Figure 4.9f and g).
Figure 4.8
4.4.3.2 Laparotomy
Jejunostomy tubes are frequently placed during a laparotomy. During laparotomy the tubes are placed either very proximal in the jejunum or distal to a surgical site to bypass it.
A #11 blade is then used to penetrate the abdominal wall from the skin surface on the right or left side of the abdominal cavity. The blade is introduced in the middle of the abdominal wall lateral to the rectus abdominalis muscle. A mosquito forceps grabs the blade in the abdominal cavity. The blade is withdrawn from the abdominal wall with the forceps. The forceps then grabs the feeding tube and pulls inside the abdominal cavity ( Figure 4.10a).
A purse‐string suture with 4‐0 monofilament absorbable suture is placed in the wall of the jejunum.
A puncture is made in the center of the purse‐string in the wall of the jejunum ( Figure 4.10b). The jejunostomy tube is then introduced in the lumen of the jejunum in the aboral direction. The tube is advanced over 20 cm and the purse‐string is tightened ( Figure 4.10c). Four pexy sutures are placed between the wall of the jejunum and the transverse abdominalis muscle around the jejunostomy tube ( Figure 4.10d and e). A 4‐0 monofilament absorbable suture is used for the pexy sutures. A finger‐trap suture with 3‐0 nylon is placed on the skin to secure the tube ( Figure 4.10f).
The laparotomy is closed in a routine fashion.
4.4.4 Tips
An 8 Fr feeding tube can be used in cats as well as in small breed dogs. The larger tube will have less change to get occluded. It is important to flush the tube regularly.
The author has not been created a tunnel between the sero‐muscularis and the submucosa to place the jejunostomy tube.
A interlock box suture technique has been described to pexy the jejunum to the abdominal wall (Daye et al. 1999).
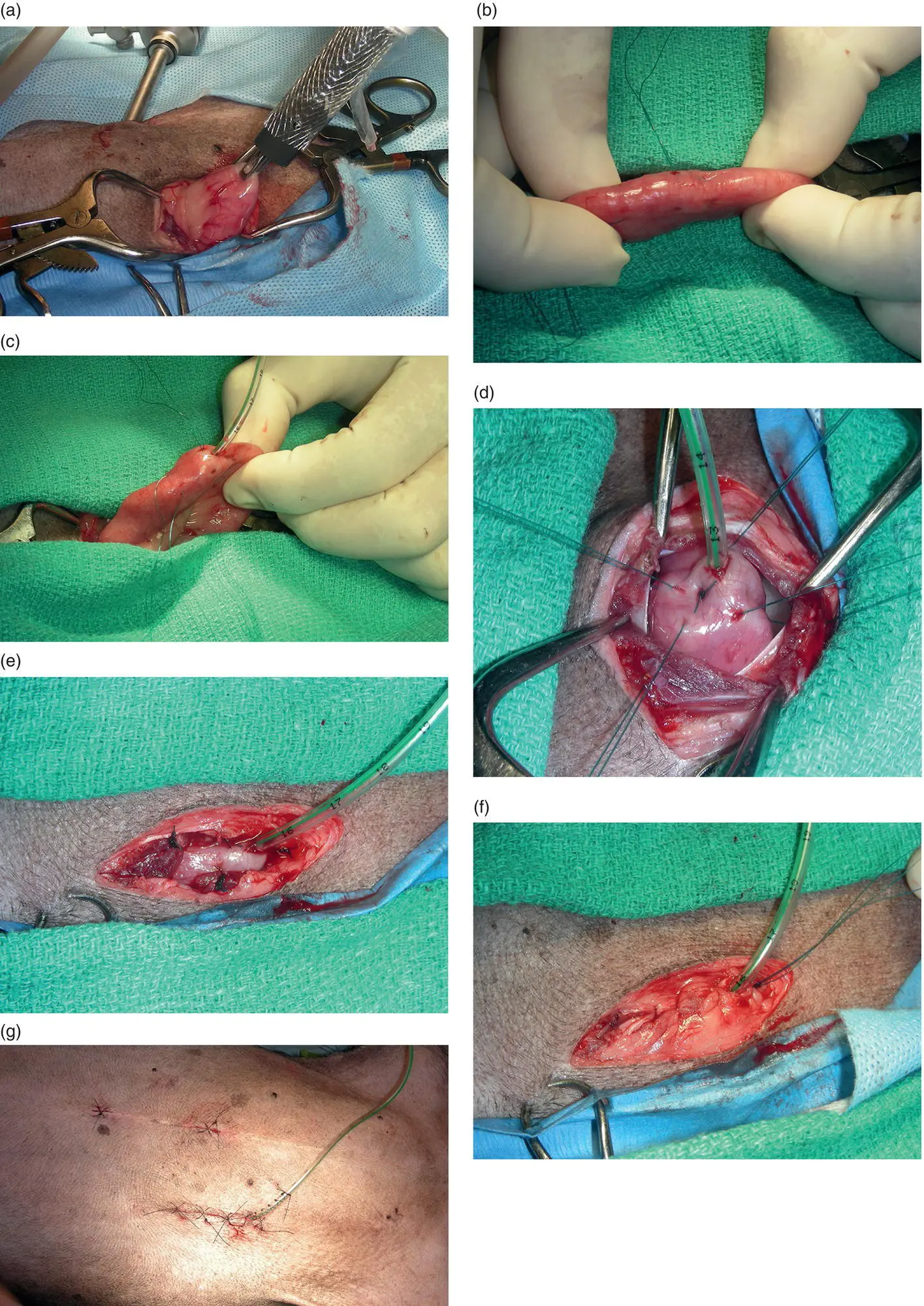
Figure 4.9
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Gastrointestinal Surgical Techniques in Small Animals»
Представляем Вашему вниманию похожие книги на «Gastrointestinal Surgical Techniques in Small Animals» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.




Обсуждение, отзывы о книге «Gastrointestinal Surgical Techniques in Small Animals» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.