Gastrointestinal Surgical Techniques in Small Animals
Здесь есть возможность читать онлайн «Gastrointestinal Surgical Techniques in Small Animals» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Gastrointestinal Surgical Techniques in Small Animals
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Gastrointestinal Surgical Techniques in Small Animals: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Gastrointestinal Surgical Techniques in Small Animals»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Describes techniques for canine and feline gastrointestinal surgery in detail Presents the state of the art for GI surgery in dogs and cats Includes access to a companion website with video clips demonstrating techniques
is an essential resource for small animal surgeons and veterinary residents.
Gastrointestinal Surgical Techniques in Small Animals — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Gastrointestinal Surgical Techniques in Small Animals», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
The length of the tube is measured from the proximal part of the esophagus to the level of the 8th or 9th rib. The appropriate length is marked on the tube.
A long curved forceps is introduced through the oral cavity in the proximal esophagus ( Figure 4.4a). The tip of the forceps is palpated percutaneously in the proximal part of the neck.
A small skin incision is made over the tip of the forceps ( Figure 4.4b). It is important to tent the soft tissue of the neck while the instrument is tipped up in the neck. This minimizes the risk of stabbing the jugular vein or the carotid artery. The tip of the forceps is then exposed after incising the wall of the esophagus. The incision should be long enough to advance the tip of the forceps through the wall of the esophagus. A large incision will result in leakage of saliva around the tube in the subcutaneous area, inducing cellulitis.

Figure 4.3
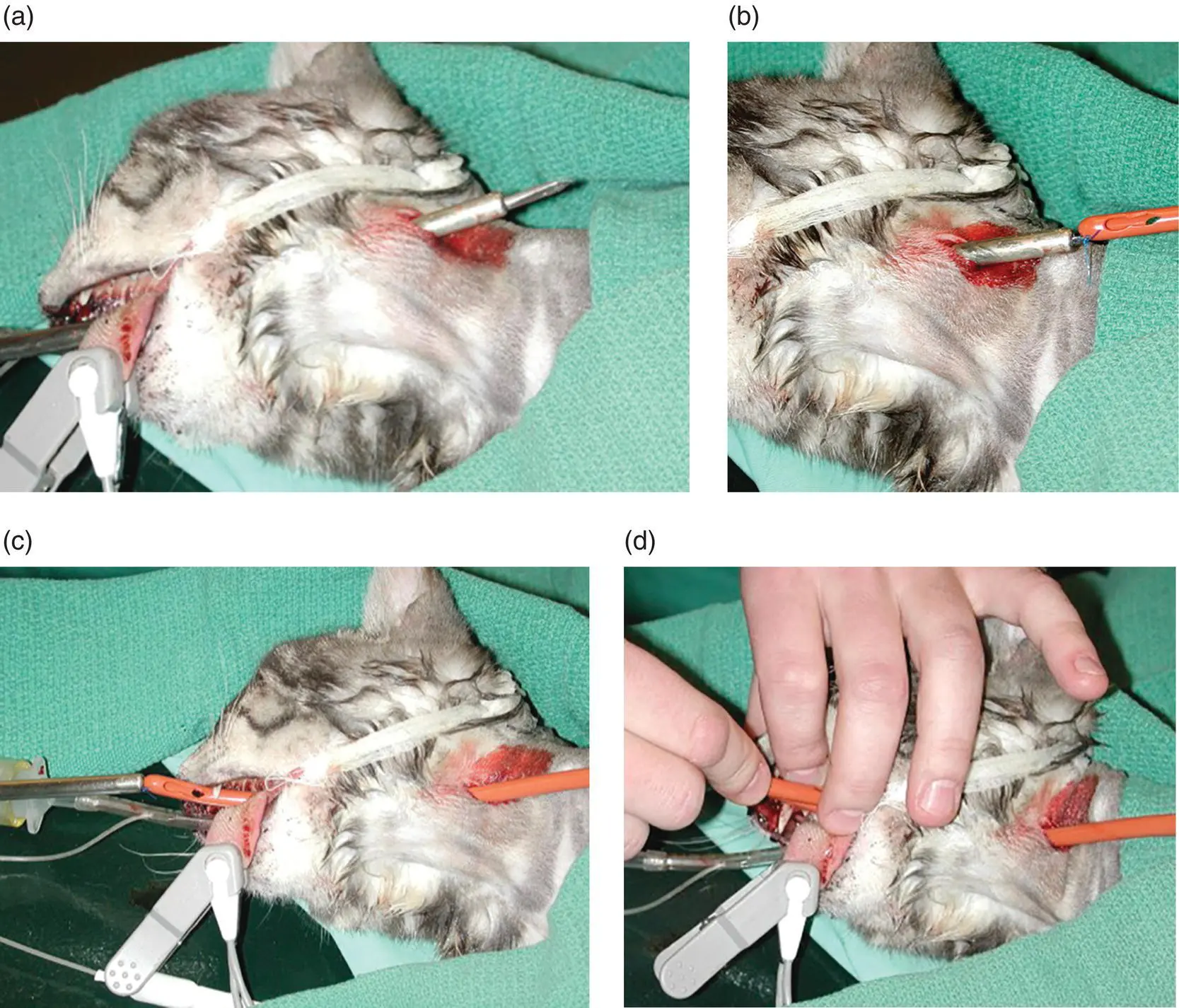
Figure 4.4
The tip of the esophagostomy tube is then grabbed and pulled in the oral cavity ( Figure 4.4b and c). The tube is then reinserted in the esophagus ( Figure 4.4d). It is important not to wrap the esophagostomy tube around the endotracheal tube. The tube is advanced until it passes the point of insertion in the esophagus. Then it can be pushed in the esophagus to the desired length.
As an alternative technique a special trocar can be used to place the esophagostomy tube. The tube is first introduced in the esophagus through the mouth ( Figure 4.5a). Then the distal end of a special curved trocar is advanced in the proximal esophagus. The skin and the wall of the esophagus are incised over the tip of the trocar ( Figure 4.5b). The esophagostomy tube is attached to the distal end of the trocar ( Figure 4.5c). The trocar is then pulled through incision in the neck, dragging the esophagostomy tube with it ( Figure 4.5d–g).
The tube is secured in placed with 2‐0 nylon suture as a Chinese finger trap (Song et al. 2008).
It is paramount that the placement of the tube is confirmed prior to feeding of the patient. A lateral radiograph is used to confirm the placement of the tip of the esophagostomy tube in the distal esophagus ( Figure 4.5g). If the tube is in the stomach, it needs to be pulled back in the esophagus.
The tube can be removed eight days after placement if it is not needed. The finger‐trap suture is just cut and the tube is pulled out. The stoma is left to heal by second intention. The dog or cat can eat immediately.
4.2.4 Tips
It is important to have an endotracheal tube to prevent placement of the tube in the airway. A long curved forceps greatly facilitates the placement of the esophagostomy tube, especially in large obese dogs. The tube should be easy to advance in the esophagus. If the tube is forced in the esophagus, there is a significant risk of perforating the esophagus at the base of the heart.

Figure 4.5
4.2.5 Utilization
Esophagostomy tube can be used right away to feed the patient. After calculation of the daily caloric requirement, the amount of food is divided in four feedings. Any diet transformed in a gruel can be used with an esophagostomy tube. The gruel is delivered slowly over 5–10 minutes to prevent vomiting. The tube is then flushed with saline to prevent obstruction.
4.2.6 Complications
Esophagostomy tubes can be dislodged or kinked if the patient is vomiting. Laceration of the jugular vein and/or the carotid artery can happen with sharp dissection. Inflammation at the stoma is frequent. It may result in mild exudate. Obstruction of the tube can occur. It is important to flush the tube with saline regularly.
4.3 Gastrostomy Tube
4.3.1 Indications
Gastrostomy tubes are used in anorexic patients. They are used to bypass the oral cavity and the esophagus because of disease process, trauma, or obstruction (Armstrong et al. 1990a; Armstrong and Hardie 1990b; Bright et al. 1991; Marks 1998).
Gastrostomy tube can be kept for long‐term support of dogs and cats. It is not unusual to have tube in place for four months. Low‐profile gastrostomy tubes are then very appropriate for long‐term support. Low‐profile gastrostomy tubes are less bulky and have more likely less chance to be pulled accidentally by the dog or the cat (Yoshimoto et al. 2006).
4.3.2 Materials and Equipment
Large‐bore feeding tube can be used for gastrostomy tube. Usually a 20–30 Fr tube can be placed. Either a Foley catheter or a mushroom‐tipped tube are used in dogs and cats ( Figure 4.6). The balloon of a Foley catheter has a tendency to rupture quickly because of the acidic environment. Mushroom‐tipped tubes are commonly use if long‐term utilization is anticipated. A low‐profile gastrostomy tube with a mushroom‐tipped can also be used.

Figure 4.6
Gastrostomy feeding tubes can be placed surgically during a laparotomy or percutaneously with endoscopy (Armstrong et al. 1990a, Armstrong and Hardie 1990b, Bright et al. 1991, Marks 1998). General anesthesia is required for the placement of a gastrostomy tube. The tubes are placed in the left side of the abdominal cavity into the body of the stomach.
4.3.3 Technique
4.3.3.1 Endoscopic Placement
Endoscopic placement of gastrostomy is recommended for patients not undergoing laparotomy. Endoscopic placement is contraindicated for patients with esophageal stricture.
The patient is placed in right lateral recumbency. A flexible endoscope is advanced in the stomach. After sufficient insufflation of the stomach an 18 gauge over‐the‐needle catheter is placed percutaneously in the lumen of the stomach. A suture is then threaded in the catheter. A snare or a grasping forceps can grab the suture in the lumen of the stomach. The suture is then pulled out through the esophagus and the mouth of the patient. The suture has to be long enough to exit in the oral cavity and still be present through the abdominal wall. Another over‐needle catheter is threaded over the suture and the gastrostomy tube securely attached to the suture. The proximal end of the gastrostomy tube is wedged in the flared end of the over‐needle catheter. A mushroom‐tipped catheter is used. The suture is then pulled from the abdominal wall to bring the gastrostomy tube in the lumen of the stomach. A small skin incision is made to facilitate the passage of the catheter through the abdominal wall. A Chinese finger‐trap suture with 2‐0 nylon is then used to secure the gastrostomy tube to the skin (Song et al. 2008). The endoscope can be reintroduced to confirm appropriate placement of the gastrostomy tube.
4.3.3.2 Surgical Placement
4.3.3.2.1 Laparoscopically Assisted
A single‐access port is inserted in the left side of the abdominal cavity caudal to the last rib. The port is placed lateral to the rectus abdominal muscle. After insufflation of the abdominal cavity a 5 mm rigid endoscope and 5 mm grasping forceps are used to visualize and grab the wall of the body of the stomach toward the fundus between the lesser and greater curvature. The stomach is brought against the abdominal wall and the single‐access port is removed. Small Gelpy retractors are used to keep the incision through the abdominal wall opened. A stay suture is placed in the wall of the stomach. A 3‐0 monofilament absorbable suture is then used to place a purse‐string suture in the wall of the stomach. A #11 blade is used to puncture the center of the purse‐string suture. The gastrostomy tube is then introduced in the lumen of the stomach. The purse‐string suture is tightened around the tube. If a Foley catheter has been used, the balloon is inflated with 5 ml of saline. Four pexy sutures are placed between the wall of the stomach and the transverse abdominalis muscle. A 3‐0 monofilament absorbable suture is used for the pexy. Another purse‐string suture is placed in the transverse abdominalis muscle around the tube to prevent its displacement. The subcutaneous tissue and skin are closed in a routine fashion around the tube. A Chinese finger‐trap suture with 2‐0 nylon is placed on the skin to secure the tube (Song et al. 2008).
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Gastrointestinal Surgical Techniques in Small Animals»
Представляем Вашему вниманию похожие книги на «Gastrointestinal Surgical Techniques in Small Animals» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.




Обсуждение, отзывы о книге «Gastrointestinal Surgical Techniques in Small Animals» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.