Gastrointestinal Surgical Techniques in Small Animals
Здесь есть возможность читать онлайн «Gastrointestinal Surgical Techniques in Small Animals» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Gastrointestinal Surgical Techniques in Small Animals
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Gastrointestinal Surgical Techniques in Small Animals: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Gastrointestinal Surgical Techniques in Small Animals»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Describes techniques for canine and feline gastrointestinal surgery in detail Presents the state of the art for GI surgery in dogs and cats Includes access to a companion website with video clips demonstrating techniques
is an essential resource for small animal surgeons and veterinary residents.
Gastrointestinal Surgical Techniques in Small Animals — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Gastrointestinal Surgical Techniques in Small Animals», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
2.1.8 Biofragmentable Anastomosis Ring
The Bowel Anastomosis Ring (BAR) (Valtrac, Medtronic, Minneapolis, MN) is a biofragmentable medical device made of two interconnecting half‐shells made of polyglycolic acid and barium sulfate ( Figure 2.1). The device is designed to facilitate anastomosis of the inverted ends of bowel without suturing. The device is placed without an incision in the cecum or retrograde placement through the rectum. It has been reported for use in human and veterinary colonic anastomoses, but also in small bowel and esophagogastric anastomoses (Corman et al. 1989; Thiede et al. 1998; Ryan et al. 2006). Its size range (21–34 mm) generally limits its use in small animal surgery for colonic and rectal anastomosis in larger breed dogs. Purse‐string sutures are placed with a Furniss clamp at the ends of bowel to be connected and the affected bowel is resected. The purse‐string sutures are tightened individually over the middle of the two interconnecting half‐shells of the BAR. The half‐shells are compressed together and intestinal continuity is restored. The rings gradually dissolve and are shed into the bowel for evacuation. The rate of leakage and stricture formation associated with the BAR is comparable to that reported in the literature for stapled and hand‐sewn colon repairs in humans (Corman et al. 1989). The BAR has been used with success in cats with megacolon (Ryan et al. 2006). The presence of the megacolon allows placement of a 25 mm BAR with 1.5 mm gap between the two‐half after compression. Relaxation of the wall of the colon to facilitate placement of the BAR can be induced with warm saline irrigation, application of topical 1% lidocaine or with IV glucagon (Hardy et al. 1987).
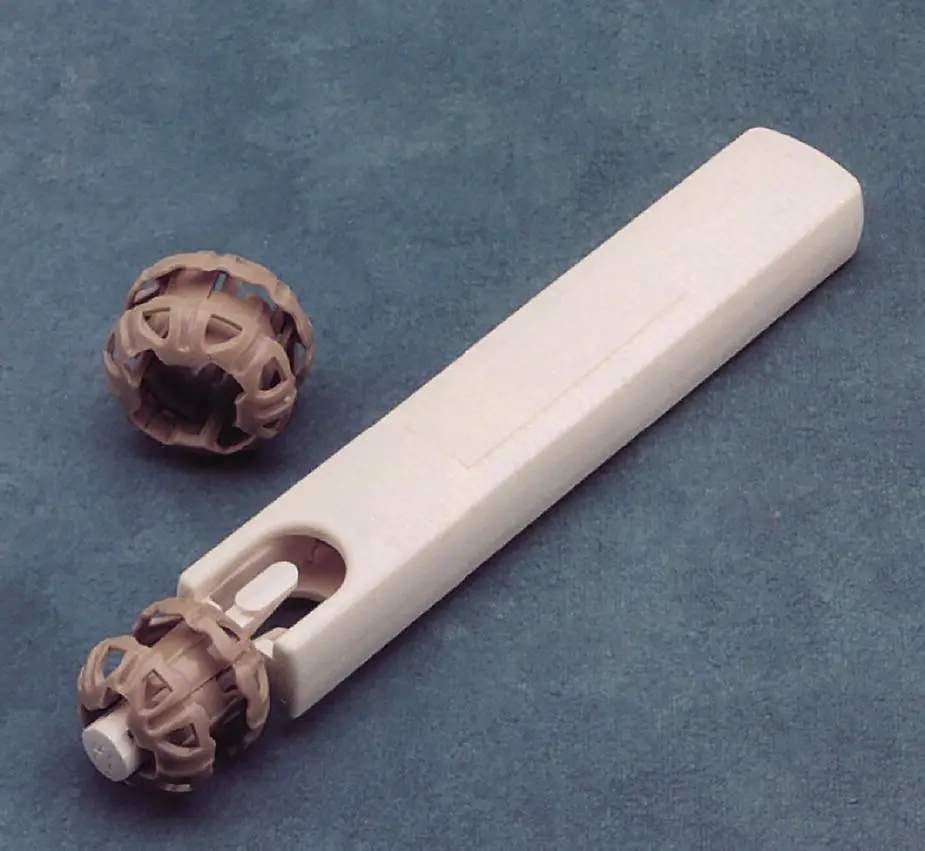
Figure 2.1
2.2 Staplers, Linear, Circular, Skin Staples
Surgical staples have been used in virtually all aspects of gastrointestinal surgeries.
Staple height is the length of the legs of the staple after trigger closure. Choosing the proper staple leg length is critical because staple legs that are too short do not engage the opposing tissue plane properly or may occlude the intramural blood supply, and choosing legs that are too long may produce ineffective closure, with subsequent leakage of bowel contents or hemorrhage. Surgeons should inspect the thickness of the tissues before choosing the appropriate stapler cartridge (staple height), since edema, and thickened and inflamed intestinal wall, may prevent proper tissue closure with staples. Different stapler configurations have been developed for gastrointestinal stapling by lot of different companies. The author is mostly familiar with the stapling from Medtronics therefore will refer to their product for the remaining of the chapter.
Surgical staplers are classified as “skin” staplers, linear staplers, and circular or end‐to‐end staplers. Skin staplers have been successfully used in single‐layer, noncrushing appositional small intestinal anastomosis, enterotomy closure, and gastropexy techniques (Coolman et al. 2000). For intestinal use, regular‐size disposable skin staplers using stainless steel staples (4.7 mm H × 3.5 mm W) (Autosuture Premium 35, Medtronics, Minneapolis, MN) ( Figure 2.2) have been reported. For gastropexy, a wide skin stapler has been recommended (Royal 12 W 6.5 mm × 4.1 H) (Coolman et al. 1999).

Figure 2.2
Linear stapling devices come in a variety of lengths and staple rows. Most linear staplers for veterinary medicine have staple height that is predetermined based on cartridge selection. Some are disposable while others come with reloadable handles with disposable cartridges. In veterinary medicine linear staplers are used most frequently for liver lobectomy, gastrotomy, gastrectomy, and bowel closure. Thoraco‐abdominal staplers (TA stapler, Medtronic, Minneapolis, MN) are common linear staplers supplied with double or triple staple rows ( Figure 2.3). Non‐cutting linear staplers are used for partial hilar lobectomy and pancreatectomy, for gastrotomies, or to staple off intestinal ends during functional end‐to‐end stapled intestinal anastomoses. TA stapler 30 V3 fires three rows of fine staples (2.5 mm open to 1 mm closed) for secure hemostatic vascular closures at the hilus of organs (lobectomies). The double‐row TA 55 and 90 mm long (3.5 mm open to 1.5 mm closed) cartridge linear staplers are most used for intestinal surgery and partial liver or partial lung lobectomy. Double‐row TA 55 or 90 (4.8 mm open to 2.0 mm closed) staplers are used nearly exclusively for partial gastrectomies or Billroth 1 procedures. Newer DST TA linear staplers use reloadable linear cartridges with directional staple technology titanium staples. This technology uses a cross‐sectional rectangular staple wire that bends more reliably into a fully formed “B”‐shaped secure staple ( http://www.medtronic.com/covidien/en‐us/products/surgical‐stapling/open‐staplers.html).

Figure 2.3
Cutting linear staplers have a cutting blade that divides the tissue after two rows of staggered staples are fired on either side of line. The gastrointestinal staplers (GIA, Medtronic, Minneapolis, MN) are commonly used in veterinary surgery and they are 60, 80, or 100 mm long ( Figure 2.4).

Figure 2.4
Linear cutting and stapling devices are often used for pulmonary, cardiac, gastrointestinal, hepatobiliary, or reproductive applications. The staplers allow occlusion and division of tissue in a single surgical maneuver. GIA 4.8 mm staplers (4.8 mm open to 2.0 mm closed) are often used for partial gastrectomy during GDV surgery, and GIA 3.8 mm staplers (3.8 mm open to 1.5 mm closed) are used for intestinal anastomosis. Gastrointestinal staplers (Endo GIA, Medtronic, Minneapolis, MN) are used during endoscopic procedures. These cutting linear staplers have staples that continue past the cutting blade limit to ensure that incomplete incisions into vessels or hollow organs do not leak.
Circular stapling devices are used to perform end‐to‐end, end‐to‐side, or side‐to‐side anastomoses in the gastrointestinal tract. It fires a circular staggered double‐row staple line, and an inner circular cutting device creates a stoma within the circular staple line ( Figure 2.5). Circular staplers create an inverted anastomosis. Circular staplers need to be sized correctly according to the diameter of the organ, and should not be used when the combined tissue thickness is less than 1 mm or more than 2.5 mm. In small animal surgery, the 21 and 25 mm EEA devices with 3.5 or 4.8 mm staples are used most often in gastrointestinal surgeries. The device diameter must fit inside the lumen of the organ to be stapled without tension. Patient size is a limiting factor for circular staplers in small animal surgery. Generally EEAs can be used in large bowel of most small animals and only medium‐ to large‐breed dogs for the small bowel. A Furniss device is used to place a purse‐string of monofilament sutures on either side of the tubular organ ends to be anastomosed. A detachable anvil is secured with one purse‐string suture. The other end is secured in a similar fashion to the stapler head. The anvil is connected to the head and the ends are firmly brought together. After the stapler is fired a circular cutting blade cuts a donut of tissue within the circular staple line ( Figure 2.6). Always inspect the donut to be sure all layers of the bowel have been cut and there is a patent lumen.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Gastrointestinal Surgical Techniques in Small Animals»
Представляем Вашему вниманию похожие книги на «Gastrointestinal Surgical Techniques in Small Animals» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.




Обсуждение, отзывы о книге «Gastrointestinal Surgical Techniques in Small Animals» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.