Mount Sinai Expert Guides
Здесь есть возможность читать онлайн «Mount Sinai Expert Guides» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Mount Sinai Expert Guides
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Mount Sinai Expert Guides: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Mount Sinai Expert Guides»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Mount Sinai Expert Guides — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Mount Sinai Expert Guides», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
See Figure 8.1.
Prognosis
There are clinical, animal, and in vitro studies which support a pathogenic role of acute hyperglycemia by causing immune system dysfunction, coagulation abnormalities, and increasing overall mortality.
Reading list
1 Finfer S, et al. Clinical review: consensus recommendations on measurement of blood glucose and reporting glycemic control in critically ill adults. Crit Care 2013; 17(3):229.
2 Markovitz LJ, et al. Description and evaluation of a glycemic management protocol for patients with diabetes undergoing heart surgery. Endocrine Pract 2002; 8(1):10–18.
Suggested websites
http://resources.aace.com/protocols.html
Guidelines
National society guidelines
| Title | Source | Date and weblink |
| Diabetes Care in the Hospital | American Diabetes Association | 2019 https://care.diabetesjournals.org/content/42/Supplement_1/S173 |
| Insulin Infusion Guideline | Society of Critical Care Medicine | 2012 https://journals.lww.com/ccmjournal/Fulltext/2012/12000/Guidelines |
Evidence
| Type of evidence | Title | Comment |
| Clinical trial | Normoglycemia in Intensive Care Evaluation Survival Using Glucose Algorithm Regulation [NICE‐SUGAR] trial | Significantly higher 90 day mortality in intensive glucose control group compared with moderate glucose control |
| Clinical trial | Leuven Surgical Trial | Intensive glucose control significantly reduced ICU length of stay, hospital length of stay, duration of mechanical ventilation, and acute kidney failure |
Images
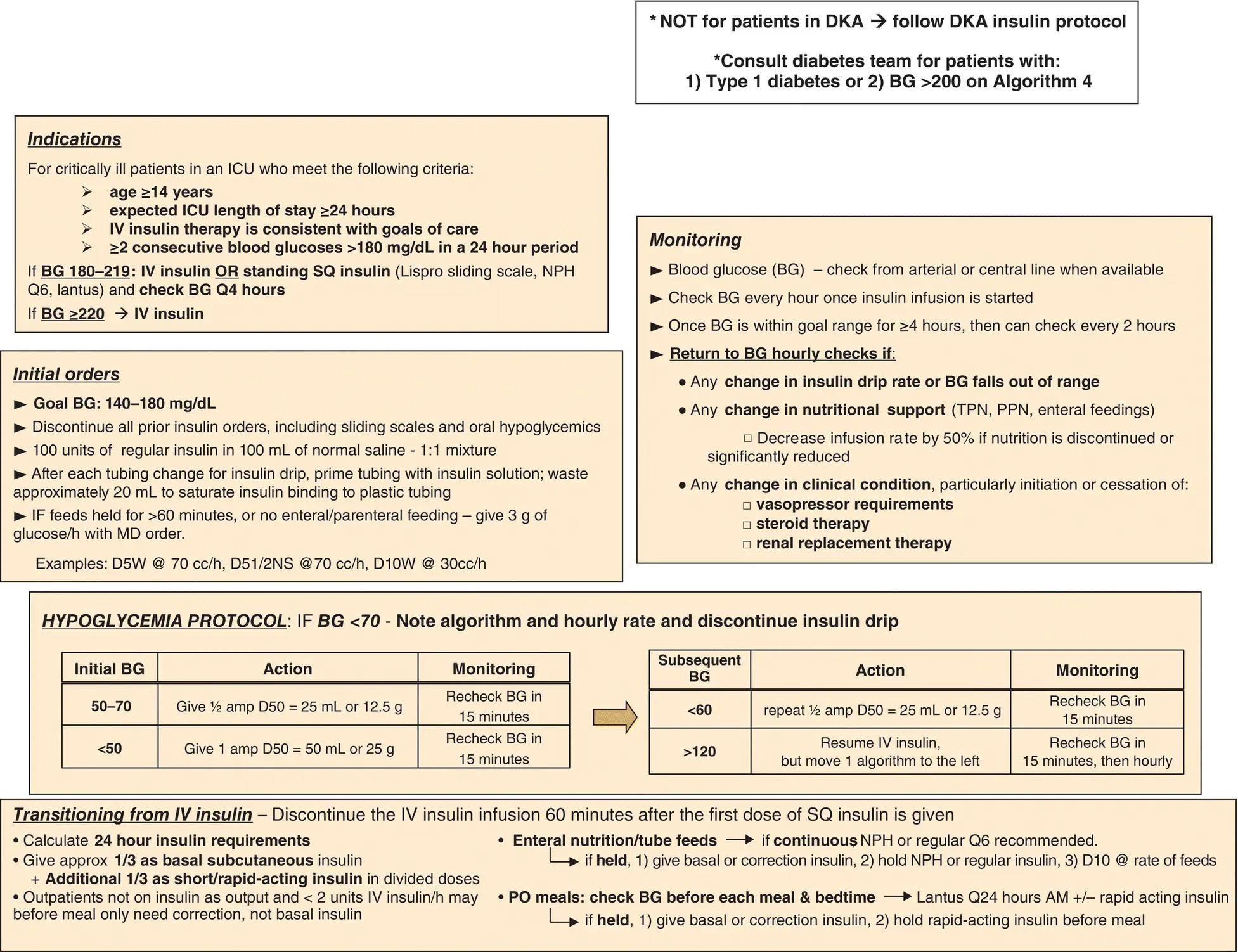
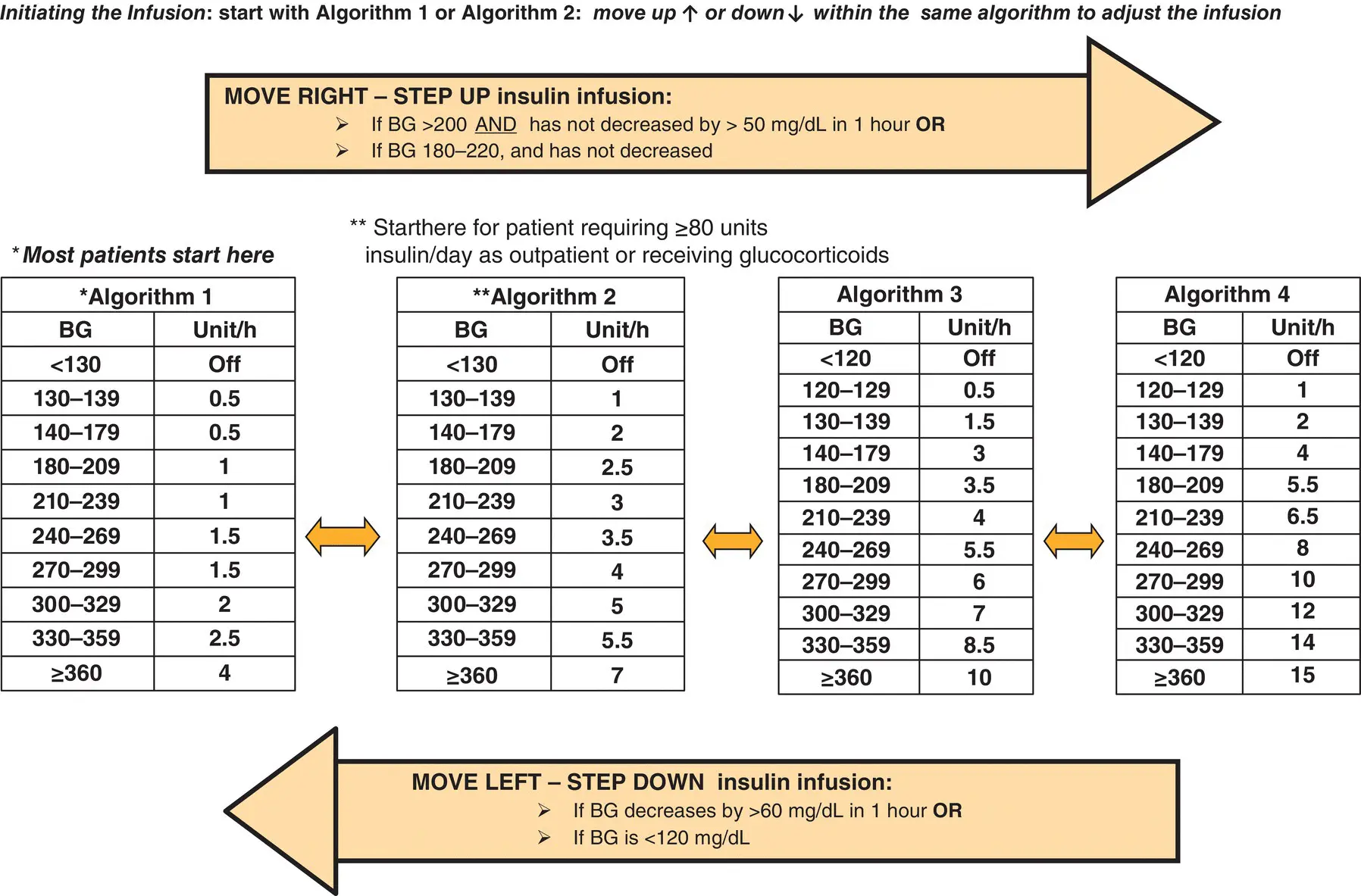
Figure 8.1 Glycemic management in critical care.
Additional material for this chapter can be found online at:
www.wiley.com/go/mayer/mountsinai/criticalcare
This includes multiple choice questions. 
CHAPTER 9 Prevention of Complications
Anthony R. Manasia and Nidhi Kavi
Icahn School of Medicine at Mount Sinai, New York, NY, USA
OVERALL BOTTOM LINE
ICU‐related complications can increase morbidity, mortality, and socioeconomic costs of the critically ill patient.
The occurrence of adverse events related to invasive procedures and medications carries significant consequences particularly in the ICU where these procedures are frequently performed.
Familiarity with specific complications and their management can help reduce the rate of adverse events.
Neurologic complications
The use of ICU pain assessment tools and daily sedation interruption have led to reduction in ICU length of stay (LOS) and patient mortality rates. The appropriate management of analgesia and sedation (see Chapter 2) can translate into significant improvements in outcome, a shortened duration of mechanical ventilation, a reduced incidence of delirium, and a reduced incidence of significant long‐term physical and cognitive dysfunction in ICU survivors.
Pain, anxiety, agitation, and PTSD have been widely studied in ventilated patients in the ICU. No one sedative agent has been reported to improve the risk of mortality among the critically ill or injured when compared in randomized control trials. For example, propofol may be associated with a shorter time to extubation and recovery from sedation when compared with midazolam. However, the risk of hypertriglyceridemia and hypotension is higher with propofol.
Propofol has also been associated with propofol‐related infusion syndrome (PRIS) which includes worsening metabolic acidosis, rhabdomyolysis, hypertriglyceridemia, hypotension, and arrhythmias. Some risk factors for PRIS are:High propofol doses.Prolonged infusion.Liver disease.Use of vasopressors.Underlying mitochondrial disease.
Dexmedetomidine has been linked to a lower risk of drug‐associated delirium than alternative sedative agents, but it increases risk of bradycardia and hypotension.
Only a minority of critically ill patients require deep sedation, for conditions such as severe respiratory failure (e.g. ARDS), intracranial hypertension, and refractory status epilepticus.
Daily sedation interruption and use of sedation scales to target light sedation have been shown to reduce ventilator time and ultimately LOS. The Richmond Agitation‐Sedation Scale (RASS) and Riker Sedation‐Agitation Scale (see Chapter 2) have the best reliability and are recommended by clinical practice guidelines.
Critical illness polyneuropathy (CIP) and myopathy (CIM) are major complications of severe critical illness and its management. CIP/CIM affects both motor and sensory axons and, as a consequence, can prolong weaning from mechanical ventilation and physical recovery. Sepsis, systemic inflammatory response syndrome, and multiple organ failure play a crucial role in CIP/CIM. Prevention of risk factors such as high dose steroids, prolonged neuromuscular blockade, prolonged immobility, treatment of the underlying critical illness, and supportive care are the mainstay of treatment. Early mobilization and physical therapy in the ICU have been shown to prevent, as well as aid in treatment of, CIP. Early rehabilitation in the ICU is safe and associated with several benefits, including improvements in muscle strength, functional mobility, quality of life, and reduction in ICU delirium.
Cardiovascular complications
Cardiovascular complications such as myocardial ischemia and cardiac arrhythmias pose an acute and life‐threatening risk to ICU patients. Cardiac tachyarrhythmias can arise from a patient's intrinsic cardiac disease, or from medications. Hemodynamic monitoring is essential in the ICU for careful patient management and to determine the etiology of changes in cardiac performance.
Bedside TTE use has gained popularity since the 1990s and has now become an important instrument in assessing the cause of and appropriate response to most hemodynamic disturbances.
We recommend the early use of goal‐directed bedside TTE in patients with hemodynamic instability, particularly those with increasing need of hemodynamic support to identify underlying treatable causes and help guide fluid resuscitation. Cardiac ultrasound allows intensivists to narrow the differential diagnosis and rapidly diagnose and initiate treatment.
Cardiac arrhythmias are a commonly encountered problem in the ICU. Preventable factors leading to arrhythmias include electrolyte abnormalities, catecholamine excess, and drug‐related adverse effects. Patients should be closely monitored for signs of cardiac ischemia with ECG and cardiac biomarkers. ECG monitoring for QT prolongation with close follow‐up can help in avoiding arrhythmias such as torsades de pointes.
QTc intervals should be particularly monitored in those receiving medications such as procainamide, amiodarone, certain antibiotics (erythromycin, pentamidine, ketoconazole), tricyclic antidepressants, and haloperidol.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Mount Sinai Expert Guides»
Представляем Вашему вниманию похожие книги на «Mount Sinai Expert Guides» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.











Обсуждение, отзывы о книге «Mount Sinai Expert Guides» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.