Mount Sinai Expert Guides
Здесь есть возможность читать онлайн «Mount Sinai Expert Guides» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Mount Sinai Expert Guides
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Mount Sinai Expert Guides: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Mount Sinai Expert Guides»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Mount Sinai Expert Guides — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Mount Sinai Expert Guides», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
If suspected, the patient should be placed in the Trendelenburg position, the pharynx and trachea (if possible) suctioned, and the airway secured with an ETT as soon as possible.
Therapy is typically supportive and antibiotics and bronchoscopic lavage are usually not necessary unless particulate aspiration is suspected or if signs of infection occur.
Reading list
1 Butterworth JF, Mackey DC, Wasnick JD. Morgan and Mikhail’s Clinical Anesthesiology, 5th edition. New York: McGraw‐Hill Education, 2013.
2 Cook TM. A new practical classification of laryngeal view. Anesthesia 2000; 55:274.
3 El‐Orbany M, Woehlick H, Ramez Salem M. Head and neck position for direct laryngoscopy. Anesth Analg 2011; 113:103.
4 Langeron O, et al. Prediction of difficult mask ventilation. Anesthesiology 2000; 92:1217.
5 Miller RD. Miller’s Anesthesia, 7th edition. Philadelphia: Churchill Livingstone/Elsevier, 2009.
6 Robitaille A, Williams SR, Trembaly MH, Guilbert F, Thériault M, Drolet P. Cervical spine motion during tracheal intubation with manual in‐line stabilization direct laryngoscopy: direct laryngoscopy versus GlideScope videolaryngoscopy. Anesth Analg 2008; 106:935–41.
7 Tanoubi I, Drolet P, Donati F. Optimizing preoxygenation in adults. Can J Anesth 2009; 56:449.
8 Watson CB. Prediction of a difficult intubation: methods for successful intubation. Respir Care 1999; 44:777.
Images
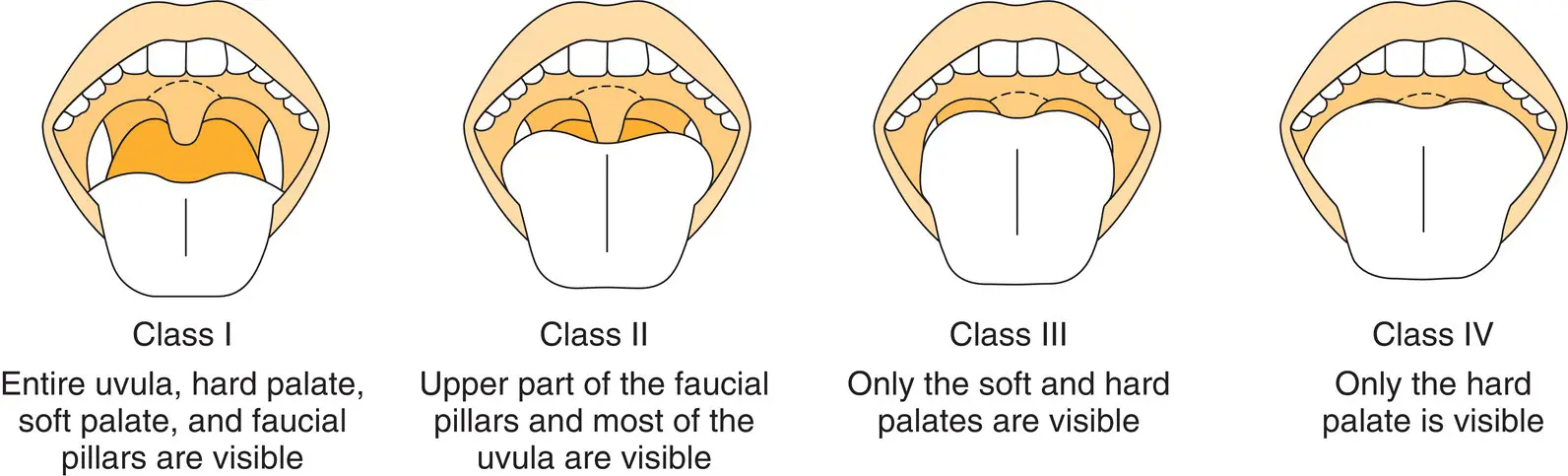
Figure 1.1 Mallampati classification.
Additional material for this chapter can be found online at:
www.wiley.com/go/mayer/mountsinai/criticalcare
This includes multiple choice questions and Video 1.1 . 
CHAPTER 2 Sedation and Analgesia
Colin J. Sheehan and Michael Kitz
Icahn School of Medicine at Mount Sinai, New York, NY, USA
OVERALL BOTTOM LINE
Analgesia and sedation are primarily indicated to prevent self‐harm and ensure the comfort of a patient. Examples include intubated patients who are dyssynchronous with a ventilator, those with open wounds postoperatively, and patients who are unable to have their pain controlled by less intensive measures.
Post‐traumatic stress disorder (PTSD) has been found in 20% of patients after discharge from an ICU. Appropriately targeted sedation therapy has been associated with decreased rates of PTSD.
‘Sedation vacations’ are associated with shorter length of ICU stay, fewer days on a ventilator, improved return to independent function at discharge, and trend toward lower ICU mortality.
Pain is experienced at greater rates among the critically ill than among the wider population. Up to 70% of patients will experience moderate to severe pain during their ICU stay. Rates have been measured up to 30% while at rest and the majority will experience pain during routine cleaning and nursing interventions.
Experiencing pain in the ICU has been associated with greater levels of chronic pain in the post ICU setting and of PTSD.
Analgosedation, or the practice of first treating with analgesics before actively sedating the patient with hypnotics, has been linked to shorter ICU length of stay and decreased duration of mechanical ventilation.
Clinical pharmacology
Context‐sensitive half‐time (CSHT) is defined as the duration of time required for plasma concentrations of a drug to decrease by 50% after discontinuing administration of the drug. ‘Context’ is meant to refer to the duration of time that an infusion has been running.
The CSHT is often different from the elimination half‐time and explains differences in duration of effect that exist based on how long an infusion is running versus the effect we see with a single bolus dose of a medication. As an example, if we were to believe that elimination half‐time determined the duration of effect of propofol, then a single bolus should leave our patient obtunded for several hours. Instead we know that a single bolus will wear off in a few minutes due to redistribution of the medication out of the central compartment into the periphery.
Likewise, the CSHT also explains why medications take longer for their effects to wear off after longer infusions. A simplified, if not perfectly scientific, explanation is that anesthetic drug effects wear off as medications redistribute from the central to the peripheral compartments. However, over time, the peripheral compartments can approach saturation, causing the central compartment to refill or maintain a steady state as its concentration decreases. Each drug has a different volume of periphery that it can fill at a different rate. Accordingly, we see that a medication like remifentanil which has virtually no CSHT will wear off in a few minutes regardless of the administration duration, while midazolam may take days after a sufficiently long infusion.
Monitoring
Sedation
Two methods have been well validated for monitoring sedation levels with equivalent results:The Richmond Agitation‐Sedation Scale ( Table 2.1) extends from –5 (unarousable) to +4 (combative) with zero representing a calm and alert patient. A typical goal is a light sedation of –1 to –2.The Riker Sedation‐Agitation Scale ( Table 2.2), extends from 1 (unarousable) to 7 (dangerous agitation), with 4 representing the calm and alert patient. A typical goal is a light sedation of 3.
Objective monitoring modalities such as EEG, bispectral index, or patient state index are not recommended by the Society of Critical Care Medicine guidelines as a regular monitoring tool. However, if the patient is paralyzed (through neuromuscular blockers or clinical condition), then use of an objective monitoring device is suggested.
Table 2.1 Richmond Agitation‐Sedation Scale.
| Score | Term | Description |
|---|---|---|
| 4 | Combative | Overtly combative or violent; immediate danger to staff |
| 3 | Very agitated | Pulls on or removes tube(s) or catheter(s) or has aggressive behaviour toward staff |
| 2 | Agitated | Frequent non‐purposeful movement or patient–ventilator dyssynchrony |
| 1 | Restless | Anxious or apprehensive but movements not aggressive or vigorous |
| 0 | Alert and calm | |
| –1 | Drowsy | Not fully alert, but has sustained (more than 10 seconds) awakening, with eye contact, to voice |
| –2 | Light sedation | Briefly (less than 10 seconds) awakens with eye contact to voice |
| –3 | Moderate sedation | Any movement (but no eye contact) to voice |
| –4 | Deep sedation | No response to voice, but any movement to physical stimulation |
| –5 | Unarousable | No response to voice or physical stimulation |
Table 2.2 Riker Sedation‐Agitation Scale.
| Score | Term | Description |
|---|---|---|
| 7 | Dangerous agitation | Pulling at endotracheal tube, trying to remove catheters, striking staff |
| 6 | Very agitated | Does not calm down despite verbal instructions, requires physical restraints |
| 5 | Agitated | Anxious or mildly agitated, calms with verbal instructions |
| 4 | Calm and cooperative | Arouses easily and follows commands |
| 3 | Sedated | Does arouse to verbal or physical stimulus, able to follow simple commands |
| 2 | Very sedated | Does not follow commands but arouses to physical stimulation |
| 1 | Unarousable | Little or no response to noxious stimuli |
Pain
Интервал:
Закладка:
Похожие книги на «Mount Sinai Expert Guides»
Представляем Вашему вниманию похожие книги на «Mount Sinai Expert Guides» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.











Обсуждение, отзывы о книге «Mount Sinai Expert Guides» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.