Biological Mechanisms of Tooth Movement
Здесь есть возможность читать онлайн «Biological Mechanisms of Tooth Movement» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Biological Mechanisms of Tooth Movement
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Biological Mechanisms of Tooth Movement: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Biological Mechanisms of Tooth Movement»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
delivers a comprehensive reference for orthodontic trainees and specialists.
It is fully updated to include new chapters on personalized orthodontics as well as the inflammatory process occurring in the dental and paradental tissues. It is heavily illustrated throughout, making it easier for readers to understand and retain the information discussed within. The topics covered range from bone biology, the effects of mechanical loading on tissues and cells, genetics, tissue remodeling, and the effects of diet, drugs, and systemic diseases.
The Third Edition of
features seven sections that cover subjects such as:
The development of biological concepts in orthodontics, including the cellular and molecular biology behind orthodontic tooth movement Mechanics meets biology, including the effects of mechanical loading on hard and soft tissues and cells, and biological reactions to temporary anchorage devices Inflammation and orthodontics, including markers for tissue remodeling in the gingival crevicular fluid and saliva Personalized diagnosis and treatment based on genomic criteria, including the genetic influences on orthodontic tooth movement Rapid orthodontics, including methods to accelerate or decelerate orthodontic tooth movement Perfect for residents and PhD students of orthodontic and periodontal programs,
is also useful to academics, clinicians, bone biologists, and researchers with an interest in the mechanics and biology of tooth movement.
Biological Mechanisms of Tooth Movement — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Biological Mechanisms of Tooth Movement», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
(Source: Japp Maltha.)
In fact, this pattern of OTM concurs with the three phases described by Burstone (van Leeuwen et al ., 1999; Von Böhl et al ., 2004a, 2004b).
If the force application is discontinued because the tooth is in its desired position, the tooth tends to move in the opposite direction. This process is called relapse and can be prevented by stabilizing the tooth in its position by a retention appliance (van Leeuwen et al ., 2003; Littlewood et al., 2017).
Cell biological processes during initial phase and hyalinization
The initial phase is completely determined by the biophysical properties of the PDL (van Driel et al ., 2000; Jónsdóttir et al ., 2006). In the first few seconds the tooth moves at a rate of approximately 10 μm/s, in the subsequent 20 seconds at a rate of approximately 1 μm/s, and thereafter at 0.1 μm/s or less. It stabilizes within 5 hours. In the initial few seconds the movement is determined by a rapid reallocation of fluid, and the remaining movement indicates the viscoelastic behavior of the ECM of the PDL (van Driel et al ., 2000; Jonsdottir et al ., 2006, 2012) ( Figure 3.4).
As a result, blood vessels in the PDL are occluded, causing hypoxic conditions. This causes local cell death through the loss of cell membrane integrity and an uncontrolled release of organelles and debris into the ECM, with cell‐free areas as a result.
The necrotizing tissues initiate an inflammatory response through the action of inflammatory mediators such as interleukin‐1β (IL‐1β) and PGE2 in the surrounding tissue, which attract leukocytes and nearby phagocytes, such as macrophages and foreign body giant cells. These cells eliminate the dead cells and debris by phagocytosis (Murdoch et al ., 2004). Also, the ECM changes by protein denaturation. This means that the secondary and tertiary structures of the collagen type I fibers, for example, are lost but their primary structures remain. Therefore, the proteins can no longer perform their function, and a gelatinous (gel‐like, hyaline) substance is formed. This process in called hyalinization and is mediated by enzymes from the matrix metalloproteinase family (MMP‐1, MMP‐8, MMP‐13). Furthermore, osteoclasts migrate to the area from nearby marrow spaces, after having resorbed the bone immediately adjacent to the necrotic PDL area, in a process known as undermining resorption (Krishnan and Davidovitch, 2006; von Böhl and Kuijpers‐Jagtman, 2009), This process is enabled by the mechanosensory action of the lacuna–canalicular system in the alveolar bone. OTM becomes only possible after all necrotic tissue has been removed. Because it is almost impossible to avoid blood vessel occlusion completely, hyalinization, and the subsequent interruption of tooth movement, is a very common process.
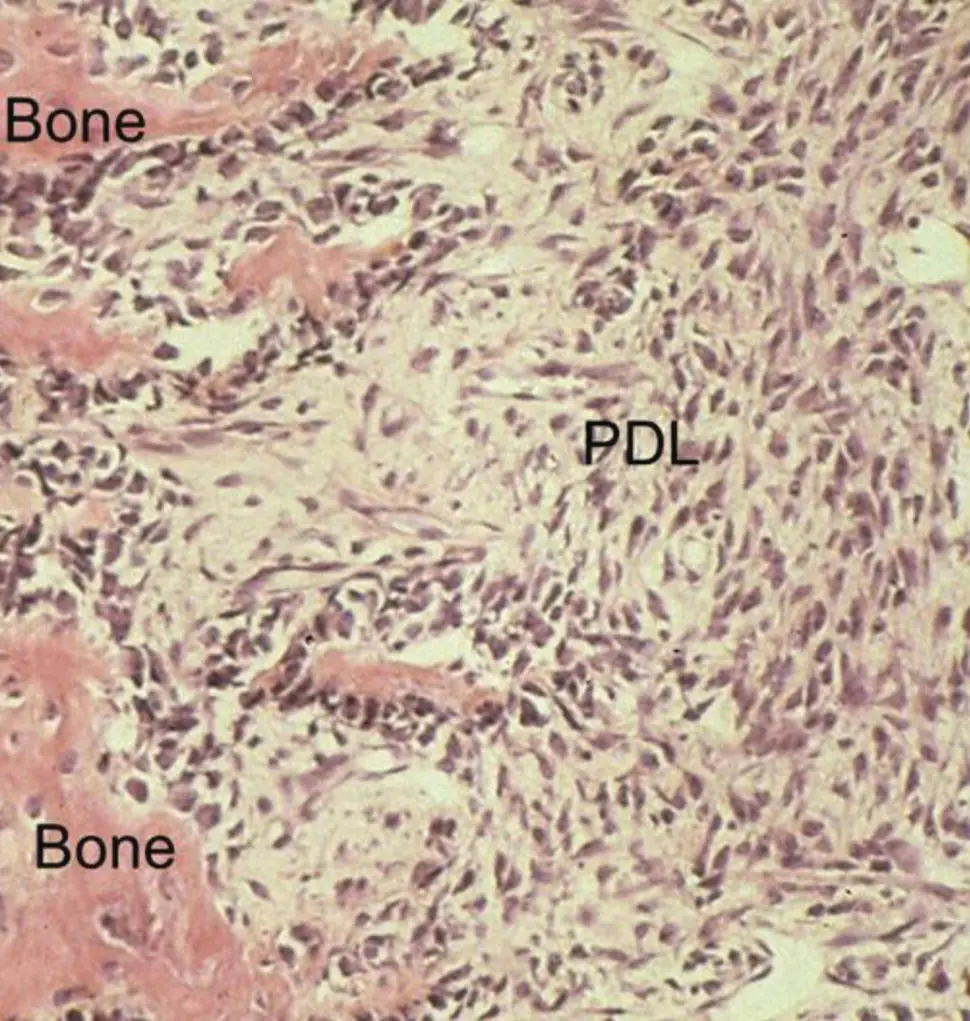
Figure 3.11 Photomicrograph of the trailing side of orthodontically moving premolar of a dog. The bone surface is covered with active osteoblasts indicating rapid bone deposition. H & E staining.
(Source: Jaap Maltha.)
The inflammatory processes related to orthodontic force application are described in detail in Chapter 4of this book.
At the trailing side of the tooth, the very fast initial movement of the tooth leads to a rapid influx of fluid in the first few seconds. In the subsequent hours, widening of the blood vessels and tensioning of the collagenous fibers are seen. During the hyalinization phase, the situation at the trailing side remains stable.
Cell biological processes during real tooth movement
At the leading side of the tooth, removal of the necrotic tissue is accompanied by an influx of differentiating fibroblasts, which secrete new ECM ( Figure 3.12). This migration is probably stimulated by periostin, an ECM protein that is expressed in periodontal tissues subjected to continuous mechanical stress (Cobo et al ., 2016).
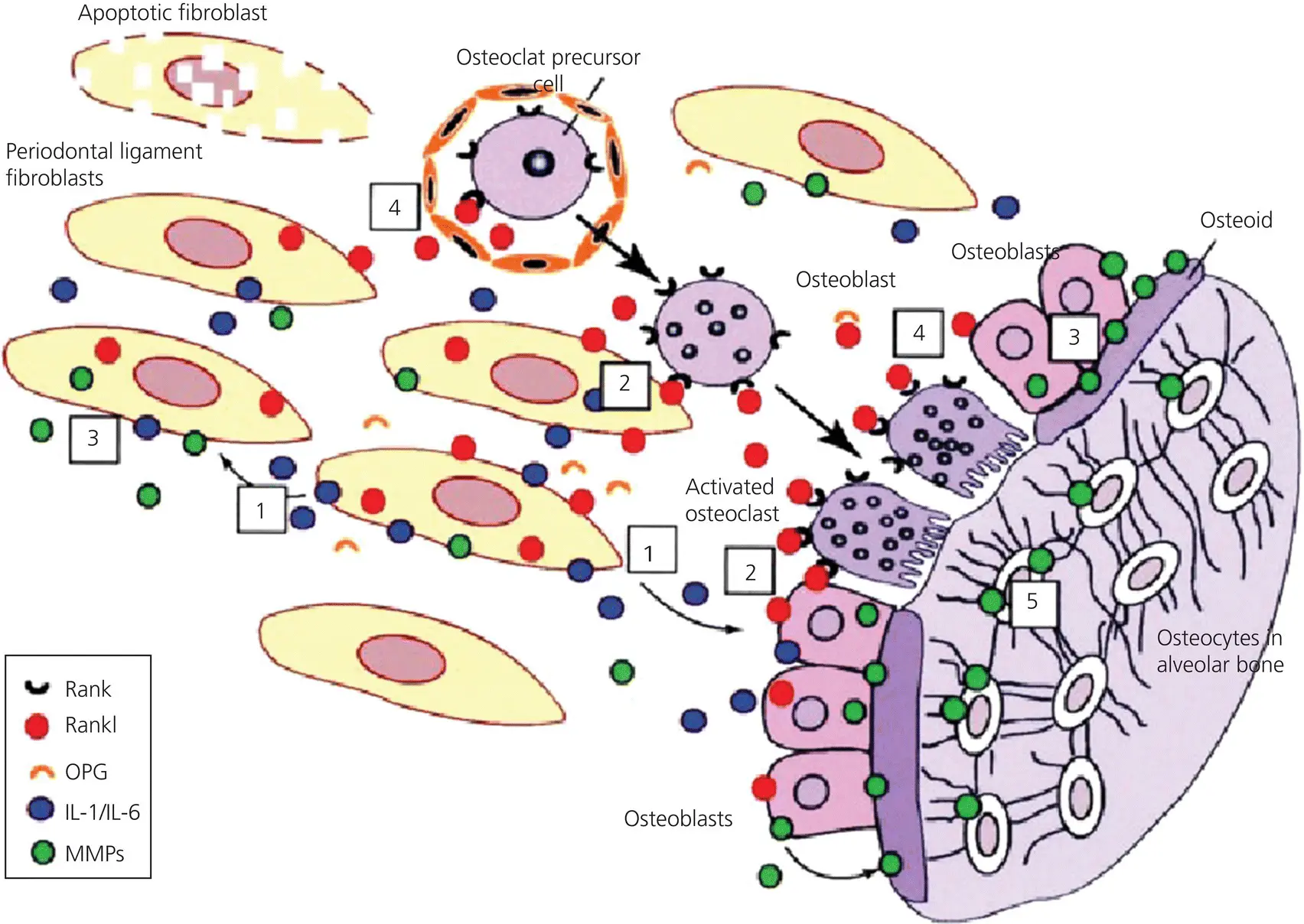
Figure 3.12 Summary of the remodeling processes at the leading side. Fibroblasts (1) under compressive strain secrete IL‐1 and IL‐6 which under these conditions upregulate the expression of the ligand for the receptor activator of nuclear factor kappa‐B (RANKL) (2) and MMPs (3) The MMPs degrade the ECM of the PDL and the osteoid (4), and RANKL stimulates the differentiation and activation of osteoclasts (5).
(Source Meikle, 2006. Reproduced with permission of Oxford University Press.)
In contrast to the normal PDL, the newly formed ECM contains mainly collagen type III instead of collagen type I. Similarly to collagen type I, type III collagen is a fibrillar collagen. It is a homotrimer containing three α1(III) chains forming a triple helix. It is rapidly produced by young fibroblasts and other mesenchymal cells in granulation tissue, and in other areas where rapid tissue formation is essential.
Simultaneously, capillaries, that are quickly recruited through endothelial cell proliferation, capillary enlargement, and elongation, restore the vasculature of the PDL. This process is mediated through VEGFs, which are synthesized and secreted by a variety of cells, such as mast cells, macrophages, and fibroblasts. Binding of circulating VEGF to VEGF receptors on endothelial cells triggers the pathway leading to angiogenesis (Salomão et al ., 2014; Tsuge et al., 2016; Militi et al ., 2019).
At the trailing side of the tooth, the proinflammatory cytokine IL‐1β and pentraxin‐ related protein (PTX3) are secreted shortly after force application by mononuclear phagocytes, fibroblasts, and endothelial cells throughout the PDL. PTX3 is involved in tissue remodeling and repair in sterile conditions (Tsuge et al ., 2016).
After the hyalinized tissue is completely removed, the tooth is again surrounded by a vital PDL. At the leading side of the tooth, the PDL contains mainly collagen type III, and at the trailing side it contains newly formed collagen type I as well as type III collagen. The orthodontic force induces negative strain at the leading side, and positive strain at the trailing side. This results in strain of the periodontal fibroblasts. The integrins by which they are attached to the ECM can act as force transducers or “strain gauges” (Chiquet et al ., 2003; Chiquet et al ., 2007). Furthermore, fluid flow in the PDL, and also within the canalicular network in the alveolar bone, is induced. In addition, this fluid flow induces strain in the cell membranes, not only of the fibroblasts, but also of the osteoblasts and the osteocytes. The osteocytes within the canaliculi of the alveolar bone are important mechanosensors and transducers of applied mechanical strain. Together with osteoblasts and periodontal fibroblasts they contribute to the activation of cells by integrin‐mediated strain transmission to the cytoskeleton and the subsequent induction of the expression of a variety of growth factors and cytokines (Klein‐Nulend et al ., 2013; Tresguerres et al ., 2020). These factors, such as FGF, IGF‐1, IL‐1α, IL‐1β, IL‐6, and TNFα mediate the differentiation of precursors into osteoblasts and osteoclasts (Eriksen, 2010; Vansant et al ., 2018).
For OTM, resorption of the alveolar bone by osteoclasts at the leading side of the tooth is essential. These cells are derived from myeloid precursors that have differentiated into monocytes and subsequently into osteoclast precursors through macrophage colony‐stimulating factor (M‐CSF). Their further differentiation is dependent on the ligand for the receptor activator of nuclear factor kappa‐B (RANKL) that is secreted by fibroblasts and osteoblasts. RANKL binds to RANK, expressed on the osteoclast precursors that subsequently become mononuclear osteoclasts, characterized by the expression of tartrate resistant acid phosphatase (TRAP). After fusion, these cells become multinuclear osteoclasts (Suda et al ., 1999; Yamaguchi, 2009; Vansant et al ., 2018). The differentiation of osteoclasts is counteracted by osteoprotegerin (OPG). This is a soluble decoy receptor for RANKL. This means that binding of OPG to RANKL inhibits the binding of RANKL to RANK on the osteoclast precursors and thus hampers both the further differentiation and the functioning of osteoclasts. Interestingly, strain affects both the secretion of RANKL and the secretion of OPG ( Figure 3.13).
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Biological Mechanisms of Tooth Movement»
Представляем Вашему вниманию похожие книги на «Biological Mechanisms of Tooth Movement» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.


Обсуждение, отзывы о книге «Biological Mechanisms of Tooth Movement» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.