Robin J. M. Gray - Temporomandibular Disorders
Здесь есть возможность читать онлайн «Robin J. M. Gray - Temporomandibular Disorders» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Temporomandibular Disorders
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Temporomandibular Disorders: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Temporomandibular Disorders»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
delivers a systematic and logical approach to diagnosing and treating temporomandibular disorders.
Using a case-based approach to assist readers with understanding and retention, the book discusses the practical realities of managing patients and promoting effective treatment of temporomandibular disorders. Containing full colour clinical images and diagrams throughout, the chapters include practical guides on how to make splints and samples of patient information sheets which can be used as templates. Readers will get access to topics such as:
The clinical aspects of anatomy, function, pathology, and classification Differential diagnosis of temporomandibular joint problems Clicking joint problems and the use of preliminary investigation in disc displacement Temporomandibular joint locking diagnosis and treatment, including final treatment plans Facial pain examinations, differential diagnosis, and questions to ask patients regarding pain in general Headaches, worn teeth, dislocated jaws, and more issues that arise in the treatment of temporomandibular joint problems Perfect for undergraduate dental students and general dental practitioners, the new edition of
is also useful to postgraduate dental students, academics, and researchers.
Temporomandibular Disorders — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Temporomandibular Disorders», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Centric occlusion and centric jaw relation 
It is important to determine whether centric occlusion (the habitual bite) coincides with centric jaw relation (the patient's relaxed mandibular position). If these two jaw positions do not coincide ( Figure 3.13), it is important to determine where the premature occlusal contact occurs at first tooth contact and what is the direction of the slide from the initial centric relation contact to the patient's habitual bite. If there is premature contact and a small slide from centric relation to centric occlusion, and if in the same sagittal plane, this is not thought to be as clinically significant as a marked lateral slide. The direction and magnitude of the slide are therefore important.

Figure 3.13The difference between (a) centric relation and (b) centric occlusion
(From Gray RJ, Davies SJ, Quayle AA. A clinical approach to temporomandibular disorders. 4. Examination of the articulatory system: the Occlusion. Br Dent J 1994;177:63–68.)
Manipulation of the mandible to centric relation is a difficult technique to master because only very gentle pressure should be applied ( Figure 3.14).
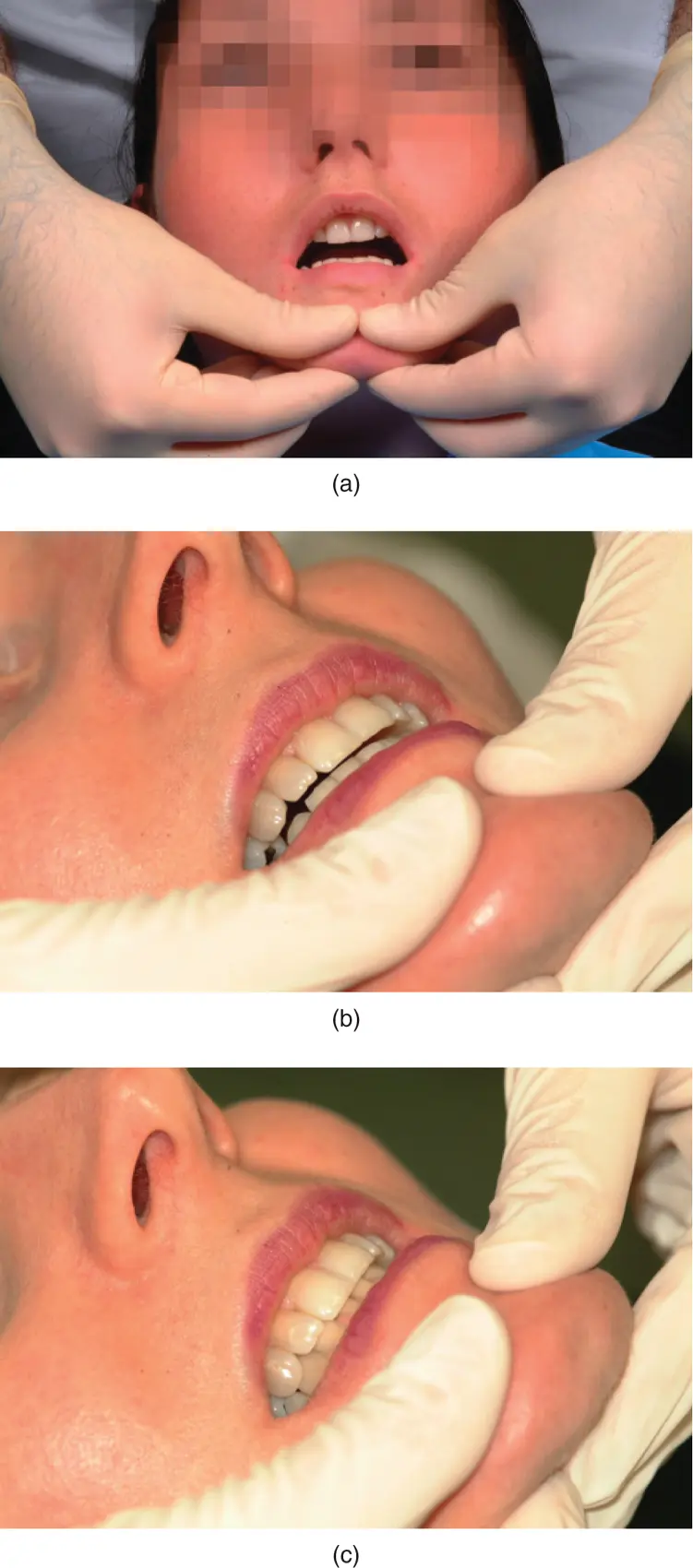
Figure 3.14(a) Centric relation (CR) recording; (b) premature contact in CR. (c) Slide from CR to centric occlusion observed and recorded.
(M. Ziad Al‐Ani, Robin J.M. Gray.)
The objective is not for the clinician to override the patient's muscle force with his or her own. If manipulation to centric jaw relation is difficult, it is sometimes useful to put a small amount of softened green‐stick compound between the upper and lower incisor teeth and help the patient to gently tap into this. This often relaxes the muscles to a degree whereby passive manipulation of the mandible can be achieved. When performing this manoeuvre, it is useful to use thin articulating paper (Baush Occlusion Paper 40 μm) supported in paper holding forceps ( Figure 3.15).
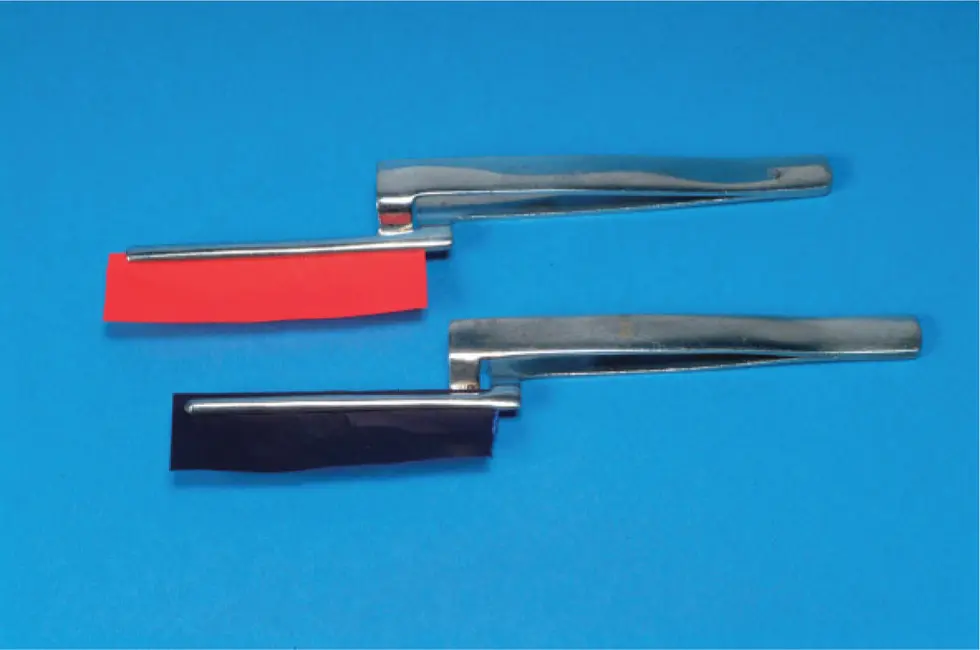
Figure 3.15Paper‐holding forceps: blue for static occlusion; red for dynamic movements.
(M. Ziad Al‐Ani, Robin J.M. Gray.)
The first tooth contact is recorded using the articulating paper and the patient is then requested to squeeze the teeth together and any slide from centric jaw relation to centric occlusion is observed and recorded.
Anterior guidance
To examine all lateral excursions, patients are instructed to close lightly into centric occlusion and subsequently slowly execute maximum active right, left, and protrusive mandibular movements while maintaining contact between the mandibular and maxillary teeth ( Figure 3.16).

Figure 3.16Determination of anterior guidance.
(M. Ziad Al‐Ani, Robin J.M. Gray.)
The anterior guidance in the mandible can be on the canine teeth, which is ideal because this means that the patient can move the mandible from side to side with immediate disclusion of the posterior teeth ( Figure 3.17).

Figure 3.17Canine guidance.
(M. Ziad Al‐Ani, Robin J.M. Gray.)
There can be group function where the canine, premolar, and molar teeth all contact during lateral excursion of the mandible. This is equally acceptable, preferably with the anterior contact being firmer than the posterior contact.
Posterior interferences
If posterior teeth ‘get in the way’ (interfere), this can be detected by immediate separation of the anterior teeth and guidance of the mandible is then transferred to the interfering tooth. It is thought that interferences, usually on the non‐working side ( Figure 3.18a) but also on the working side ( Figure 3.18b), can be responsible for initiating parafunction. Check for the presence of interferences up to maximum lateral excursions. Patients may parafunction with the mandible in very unlikely and extreme lateral positions, and this may not be clinically evident unless you are meticulous with your examination.

Figure 3.18(a) Non‐working side interference; (b) working side interference.
(From Gray RJ, Davies SJ, Quayle AA. A clinical approach to temporomandibular disorders. 4. Examination of the articulatory system: the Occlusion. Br Dent J 1994;177:63–68.)
Freedom in centric occlusion
Check whether or not the patient has freedom to move the mandible back and forward with the teeth in light contact when in centric occlusion.
Temporomandibular disorders can be initiated by restorative dental treatment. One situation is for a patient to have anterior crowns placed when he or she has a very tight anterior occlusion such as seen in a patient with an Angle's class II, division II, basal bone and incisal relationship. If crowns are placed on the upper anterior teeth, which are even marginally thicker palatally than the natural teeth were, the effect is to push the mandible distally, thereby compressing the sensitive posterior bilaminar zone of the disc and producing, sometimes severe, pain.
Record‐keeping
It is important not only for clinical reasons but also for medicolegal reasons to keep accurate and contemporaneous notes of all aspects of your clinical examinations. Remember that it may be several months or even years later when you might be asked to produce them.
Further Reading
1 Al‐Ani, M.Z. and Gray, R.J. (2004). Evaluation of three devices used for measuring mouth opening. Dent Update 31: 346–348. 50.
2 Davies, S.J. and Gray, R.J.M. (2001). The examination and recording of the occlusion: why and how. Br Dent J 191: 291–296. 299–302.
3 Gallagher, C., Gallagher, V., Whelton, H., and Cronin, M. (2004). The normal range of mouth opening in an Irish population. J Oral Rehabil 31: 110–116.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Temporomandibular Disorders»
Представляем Вашему вниманию похожие книги на «Temporomandibular Disorders» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.





![John Bruce - The Lettsomian Lectures on Diseases and Disorders of the Heart and Arteries in Middle and Advanced Life [1900-1901]](/books/749387/john-bruce-the-lettsomian-lectures-on-diseases-and-disorders-of-the-heart-and-arteries-in-middle-and-advanced-life-1900-1901-thumb.webp)
Обсуждение, отзывы о книге «Temporomandibular Disorders» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.