Practical Procedures in Implant Dentistry
Здесь есть возможность читать онлайн «Practical Procedures in Implant Dentistry» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Practical Procedures in Implant Dentistry
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Practical Procedures in Implant Dentistry: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Practical Procedures in Implant Dentistry»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
covers core topics such as:
Rationale and assessment for implant placement and restoration, including the diagnostic records and surgical considerations required for optimal planning and risk management Incision design considerations and flap management, with an essential knowledge of regional neuro-vascular structures Implant placement, encompassing the timing of the placement, bone requirements and understanding the importance of the peri-implant interface for soft tissue stability Impression techniques, loading protocols, digital workflows and the aesthetic considerations of implants Prosthetic rehabilitation of single tooth implants to fully edentulous workflows, including discussions of soft tissue support, biomechanics and occlusal verification Perfect for both general dental practitioners and specialists in implant dentistry,
is also a valuable reference to senior undergraduate and postgraduate dental students.
Practical Procedures in Implant Dentistry — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Practical Procedures in Implant Dentistry», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
The nasal cavity is very well vascularised, with the sphenopalatine artery, a branch of the internal maxillary artery, providing the largest contribution of arterial supply. It is a branch of the sphenopalatine artery that anastomoses with the greater palatine artery via the incisive canal. The nasopalatine nerve, a branch of the maxillary division of the trigeminal nerve (CN V2), provides sensory input for the nasal cavity and follows the path of the sphenopalatine artery through the incisive canal where it anastomoses with the greater palatine nerve.
7.3.1 Importance in Oral Implantology
Dental implant placement in the anterior maxilla may be limited by the position of the anterior portion of the nasal cavity, particularly when the vertical height of the residual alveolar process is reduced. In such instance, penetration of the inferior border of the nasal cavity may occur. Nasal floor augmentation (NFA) techniques utilising autogenous bone grafts, allografts, xenografts, and combination grafts have been described in the literature [6–9] as methods for managing the atrophic maxilla. Although more clinical research is needed to fully evaluate the predictability of NFA, it may provide a viable and less invasive option than a traditional Le Fort 1 osteotomy [10].
7.4 Infraorbital Foramen
The infraorbital foramen is located immediately below the inferior border of the orbit and contains the infraorbital artery and infraorbital nerve ( Figure 7.2). The infraorbital artery originates as a branch of the maxillary artery and anastomoses with the facial artery following its emergence through the infraorbital foramen. The infraorbital nerve is a terminal branch of the maxillary nerve (CN V2). It resides beneath the quadratic labii superioris and provides sensory innervation to the lower portion of the eyelid, the upper lip, and the lateral portion of the nose.

Figure 7.2 Location of the infraorbital foramen. The location of the infraorbital foramen is circled in yellow and can be found far superior to the maxillary occlusal plane.
7.4.1 Importance in Oral Implantology
Due to its superior location relative to the position of the alveolar process, the infraorbital foramen is not typically encountered in the surgical placement of dental implants. The infraorbital nerve can, however, be damaged by flap reflection and the use of retractors when performing a lateral window technique sinus lift and/or in cases of extensive maxillary ridge atrophy. Pulpal and soft tissue anaesthesia of the maxillary premolars, canine, and incisors may be achieved via the infraorbital block, which delivers anaesthetic to the infraorbital foramen as referenced 1 cm below the inferior orbital margin.
7.5 Maxillary Sinus
The maxillary sinuses are among the four pairs of paranasal sinuses (frontal sinuses, sphenoid sinuses, ethmoid sinuses, and maxillary sinuses), and the only sinuses relevant to oral implantology. The maxillary sinus expands throughout childhood, with continued inferior expansion resulting in close approximation of the sinus floor to the root apices of the maxillary premolars and molars [11]. In the event of the loss of a maxillary posterior tooth, continued sinus pneumatisation inferiorly can result in inadequate bone volume for placement of a dental implant in the alveolar process or basal bone ( Figure 7.3) [12].
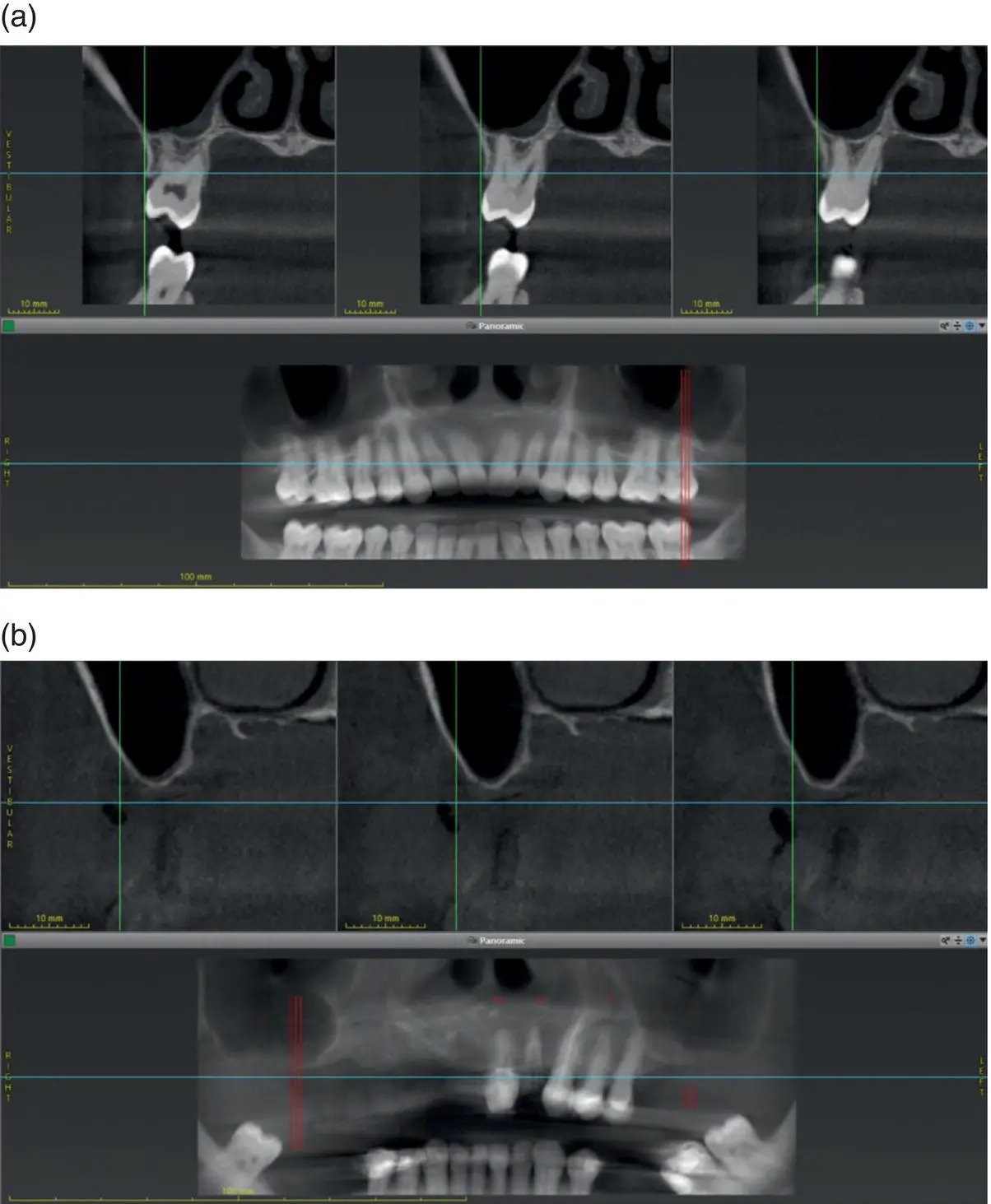
Figure 7.3 Changes in the presentation of the maxillary sinus. (a) In the dentate subject depicted in these panoramic and cross‐sectional CBCT scan views, a significant volume of bone is maintained in the alveolar process buccally, lingually, superiorly, and even inter‐radicularly. (b) In the partially edentulous subject similarly depicted, a marked loss of the alveolar process and pneumatisation of the maxillary sinus can be observed. This has resulted in an almost uniform, eggshell‐thin layer of bone separating the maxillary sinus from the oral cavity.
The maxillary sinus in adults is a hollow pyramidal shaped space in the maxilla approximately 15 mL in volume [13], roughly 3.5 cm high × 2.4 cm wide × 3.5 cm antero‐posteriorly [14]. The sinus communicates with the nasal cavity via an opening high on the medial wall of the sinus called the ostium, which is an opening approximately 3 mm in diameter [15] in the middle meatus or space located just superior to the inferior concha.
The anterior wall of the maxillary sinus is formed by the canine fossa and is close to the infraorbital foramen. The lateral wall of the sinus is formed by the zygoma. The superior wall of the sinus is the orbital floor. The posterior wall of the sinus separates the space from the structures of the infratemporal fossa and the pterygomaxillary fossa. The inferior wall or floor of the sinus is created by the alveolar process and basal bone, as well as the hard palate.
The pyramidal shape of the maxillary sinus may be further complicated or compartmentalised by the presence of bony septa, which can cause partial division of the sinus. These septa are very common and may be found in 25–33% of sinuses [16, 17]. Although numerous variations, shapes, sizes, and locations [18] may be encountered, septa tend to have a wider base inferiorly and converge to a sharp edge superiorly.
The maxillary sinus derives its sensory innervation from branches of the maxillary nerve (CN V2) via the anterior, middle, and posterior superior alveolar nerve branches as well as the infraorbital nerve. Blood supply to the sinus stems from branches of the maxillary artery, namely the infraorbital and posterior superior alveolar arteries with some contribution additionally from the sphenopalatine and posterior lateral nasal arteries. Venous drainage of the maxillary sinus occurs via the facial vein, the pterygoid plexus, and the sphenopalatine vein.
The lining of the maxillary sinus consists of a specialised pseudostratified ciliated columnar epithelium and is called the Schneiderian membrane, which in health is usually less than 1 mm thick [19]. This complex respiratory mucosa contains specialised beaker (goblet) cells that produce mucus. The mucus traps inhaled particles, keeps the surface of the membrane moist, and serves to humidify inhaled air. The ciliated columnar epithelium provide a means of transport for the produced mucus. As a functional unit, the muco‐ciliary escalator lifts the mucus secretions and small particles up to the ostium and out to the nose.
7.5.1 Importance in Oral Implantology
A frequently encountered challenge when treating the edentulous posterior maxilla with dental implants is insufficient bone volume in an area with poor bone quality [20]. The bone volume of the residual alveolar ridge available for implant placement in this region may be limited by the presence of the maxillary sinus with or without pneumatisation, the loss of alveolar bone height following tooth loss, or a combination of both [21]. Bone volume may be increased via augmentation procedures of the maxillary sinus utilising a variety of surgical techniques and grafting materials in a predictable fashion [22–24].
Current evidence suggests that both lateral sinus floor elevation (SFE) and crestal SFE techniques are both predictably successful and safe, resulting in good long‐term implant survival rates [25, 26]. Examples of lateral sinus floor elevation are depicted in Figure 7.4. The clinician may utilise parameters including residual bone height, residual bone width, length of edentulous span, and residual bone quality to help guide the selection of a lateral versus crestal SFE, as well as determining whether a simultaneous or delayed implant placement is indicated. Future research on the long‐term viability of short implants (4–6 mm) may show a decrease in the need for SFE altogether [27].
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Practical Procedures in Implant Dentistry»
Представляем Вашему вниманию похожие книги на «Practical Procedures in Implant Dentistry» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.








Обсуждение, отзывы о книге «Practical Procedures in Implant Dentistry» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.