Salivary Gland Pathology
Здесь есть возможность читать онлайн «Salivary Gland Pathology» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Salivary Gland Pathology
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Salivary Gland Pathology: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Salivary Gland Pathology»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
now features case presentations to place the information in context, as well as additional treatment algorithms in each chapter to assist in clinical decision making. Written by highly respected clinicians, educators, and researchers with extensive expertise in oral and maxillofacial surgery, this authoritative resource:
Reviews the etiology, diagnosis, and treatment of all salivary gland pathologies, with detailed explanations and hundreds of full-color clinical images Incorporates new information on the taxonomy of salivary gland tumors, neoplastic and non-neoplastic entities, image guided biopsies of salivary gland lesions, and complications in traditional and non-traditional forms of salivary gland surgery Offers expanded coverage of histopathology, including classification, grading, and staging of salivary gland tumors Features up-to-date chapters on anatomy and physiology, imaging, cysts, systemic diseases, tumors, trauma, and innovative salivary gland surgical techniques Includes a discussion of meta-analyses and systematic reviews to support evidence-based practice remains the definitive resource for oral and maxillofacial surgeons, otolaryngologists, head and neck surgeons, and general surgeons as well as their residents providing care for patients with salivary gland pathology.
Salivary Gland Pathology — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Salivary Gland Pathology», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
During sialography, there are two major phases of contrast filling: ductal and acinar. The initial or ductal phase will demonstrate the major or primary duct as well as the smaller secondary and tertiary ducts. The acinar phase is visualized as the contrast “blush” and demonstrates the parenchymal portion of the gland. Sialographic finding in obstructive disease will demonstrate the anatomy of the main, secondary, and occasionally tertiary ducts. Visualized will be strictures, obstructions, accessory glands, masses, and sialoliths. The observed obstructions include calcified and noncalcified sialoliths, mucous plugs, fibrin clots, other soft‐tissue plugs, intraductal tumors, duct stenosis and strictures, and various anatomical kinking of the ducts.
The major parenchymal disorder of salivary gland that can be identified by sialography is the acinar change seen in Sjögren syndrome ( Figure 2.23). This systemic autoimmune condition affects most of human exocrine glands but much more so the major and minor salivary glands (Golder and Stiller 2014). During the early phase of this syndrome, when imaged, these glands appear unremarkable but as Sjögren syndrome progresses, the salivary glands diffusely enlarge, mimicking chronic sialadenitis. Imaging of the salivary glands during this later time will demonstrate tiny discrete collections of contrast within the parenchyma of the salivary gland without interconnecting ducts. Advanced imaging techniques such as ultrasound, MRI, and CT have attempted to demonstrate these findings, but ultimately conventional sialography has proven to be the technique of choice for definitive imaging of patients afflicted with Sjögren syndrome.

Figure 2.23. Parotid sialogram. Note the punctate filling areas without ductal involvement. These findings are seen predominately in Sjögren syndrome patients.
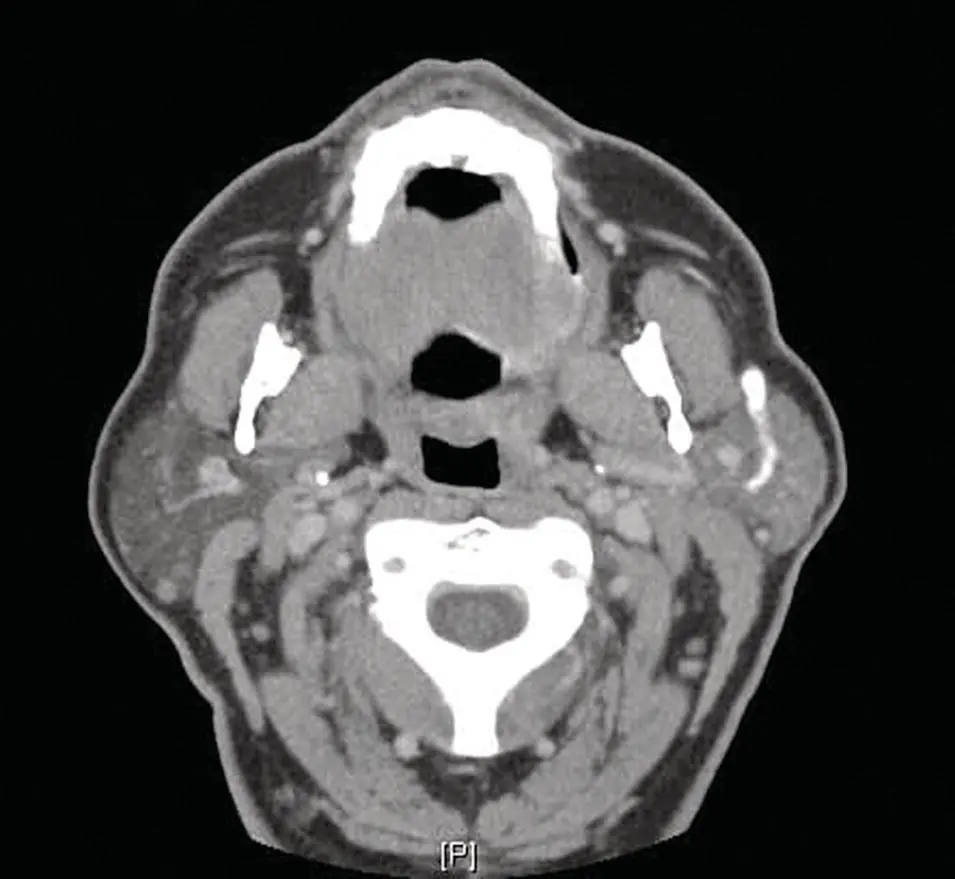
Figure 2.24. Parotid sialo‐CT. Although the main duct is opacified, it is impossible to determine areas of stenosis and/or dilatation.
In addition to conventional sialography, MR sialography, CT sialography ( Figure 2.24), and digital subtraction sialography are also available. Each of these methods attempts to better identify the primary and secondary ductal systems and thus better define the exact nature of the clinical salivary malady.
Digital subtraction sialography utilizes the images obtained from conventional sialography and masks out the underlying osseous structures by means of computer revision to better visualize the duct system. This type of examination is more time consuming and can be quite difficult to interpret except by very experienced radiographers. In addition, this technique is considerably more expensive than conventional sialography and often without significant clinical benefit.
CT sialography allows better visualization of gland parenchyma and is widely available in many larger medical centers. In this method, contrast medium is injected into the primary duct followed by a CT exam. Contemporary multi‐detector computed tomography allows reconstruction or reformatting of the original axial CT image into images representing many orthogonal planes. The major disadvantage of this method is one cannot visualize the dynamic duct filling and thus inadvertent overpressure may cause duct damage or rupture. In addition, it is very difficult to distinguish duct stenosis from anatomic variances of the normal duct system.
MR sialography (MRSIAL) appears to delineate the salivary ductal system as well as conventional sialography without the need of duct catheterization and subsequent contrast administration. Fluid‐sensitive MR sequences now obviate this clinical need. MR can detect obstructions, stenosis, and strictures of the primary, secondary, and often tertiary ducts as well as conventional sialography. In addition, advances in 3D MRI will allow the production of virtual endoscopic views from available MR data. This noninvasive procedure does not depend on operator skill for definitive imaging. By using a heavily T2 weighted sequence, hyperintense saliva is visualized within the ductal system. This salivary flow functions much as does contrast during the conventional sialogram, thus allowing the detection of morphologic ductal alterations as well as parenchymal changes. Such studies have been shown to be helpful in not only obstructive salivary gland disease but also parenchymal diseases such as Sjögren syndrome (SS) (Andre’ et al. 2021). It has been recently shown that MRSIAL is more sensitive in the detection of SS, than ultrasound (US). This technique also produces less false negatives than other imaging modalities. The major disadvantages of MRSIAL appear to be the much higher cost of both the equipment needed for the exam and the professional cost of the imaging exam itself.
IMAGE‐GUIDED BIOPSIES OF SALIVARY GLAND PATHOLOGY
Salivary gland tumors are relatively rare, yet they encompass a wide range of benign and malignant diagnoses. Even though most of the primary tumors are epithelial in origin, the histology is often very diverse and complicated. Such diversity presents a diagnostic challenge to most contemporary pathologists.
To ensure proper surgical/medical intervention, a definitive diagnosis of parotid and other salivary gland masses is essential (Haldar et al. 2016). The primary techniques involved in such undertakings include (i) preoperative needle biopsy, both fine needle or core needle; (ii) intraoperative frozen section; and (iii) open biopsy or definitive excision. Clinicians have various imaging techniques that can be employed in conjunction with these invasive diagnostic procedures.
A surgical open biopsy has historically been used for obtaining biopsy tissue and providing a microscopic diagnosis of salivary gland neoplasia. In the early and mid‐1980s, incisional biopsy of salivary gland tumors fell out of favor due to several factors including tumor seeding of the adjacent soft tissues, transient or permanent nerve damage of the facial nerve, and sialocele formation.
Needle biopsies of salivary gland, both fine needle (FNA) and core biopsies are utilized in most imaging facilities (Novoa et al. 2015). These procedures, particularly the FNA, are minimally invasive and most often will be completed with only local anesthesia. Imaging for such needle biopsies can now be accomplished with several imaging modalities including computerized tomography (CT), magnetic resonance (MR), and/or ultrasound (US). For very superficial lesions, hand‐pressure localization without concurrent imaging will also accomplish the same objective in a short period. FNA biopsies were originally used in the late 1970s and proved a safe and accurate procedure in the hands of a well‐trained cytopathology center. It has been demonstrated that such biopsies are often associated with inaccurate diagnoses outside such centers.
The most commonly performed salivary gland biopsy technique is the core needle biopsy, particularly when associated with US guidance ( Figure 2.25). This method has gained great acceptance in the pathology, imaging, and surgical arenas. Ultrasound (US) has become the preferred imaging study of choice principally because it does not produce radiation to the patient as does CT, nor is US as time consuming and expensive as MRI (Kim and Kim 2018). Currently, US imaging when used with a core needle biopsy has been proven to produce accurate diagnoses with a high sensitivity and specificity. In their meta‐analysis, Kim and Kim (2018) reviewed 10 observational studies and identified a sensitivity and specificity for the diagnosis of salivary gland pathology of 94 and 98%, respectively. Seven hematomas, one instance of temporary facial nerve paralysis thought to be caused by the local anesthesia, and no tumor seeding were reported from a total of 1315 procedures. Witt and Schmidt (2014) performed a systematic review and meta‐analysis of ultrasound‐guided core needle biopsy of salivary gland lesions. Five studies qualified for inclusion after an initial search of 7132 studies. The sensitivity and specificity of core needle biopsy were 96 and 100%, respectively in a total of 512 procedures, 88% of which were performed on the parotid gland and 12% were performed on the submandibular gland. The authors reported eight hematomas and one case of temporary facial nerve weakness secondary to local anesthesia. The authors concluded that the procedure is highly sensitive and specific and associated with a low risk of complications.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Salivary Gland Pathology»
Представляем Вашему вниманию похожие книги на «Salivary Gland Pathology» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.








Обсуждение, отзывы о книге «Salivary Gland Pathology» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.