Paul Coceancig - 6Ways to Design a Face
Здесь есть возможность читать онлайн «Paul Coceancig - 6Ways to Design a Face» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:6Ways to Design a Face
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
6Ways to Design a Face: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «6Ways to Design a Face»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
6Ways to Design a Face — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «6Ways to Design a Face», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
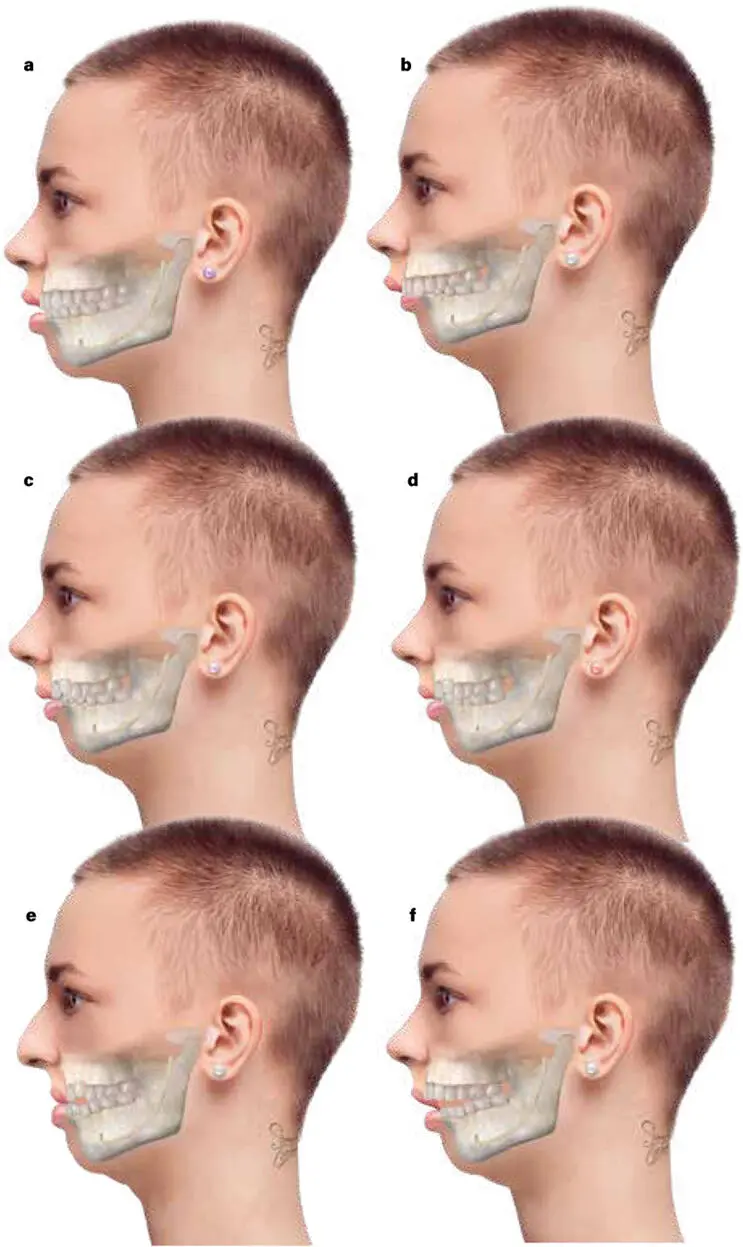
FIG 1-13 Orthognathic malocclusion series 1: Agenia, with and without AMHypo, with and without maxillary hypoplasia, looking only at the teeth and facial profile and jaw size. (a) Normally proportioned mandible and maxilla without a chin button (agenia). There is a full complement of 32 teeth in full natural occlusion. Without a natural chin button, the lips are slightly parted, and the molar and incisor occlusion is an Angle Class I without dental crowding. With the lips slightly parted, the anterior teeth are prominently seen, and the appearance is of anterior dental fullness. Orthodontically, this would be called maxillomandibular protrusion with Class I occlusion without crowding. (b) AMHypo with agenia with the maxillary arch drawn normally. The appearance is of prominent upper lip protrusion and prominent maxillary tooth display. There is significant dental overjet and deep incisor overbite. The mandibular teeth are not crowded, and the first molars are in a Class II relationship. Orthodontically this is classified as Angle Class II, division 1 malocclusion. Division 1 implies that the maxillary incisors are well forward of the mandibular incisors. (c) AMHypo with agenia with the collapse of the maxillary anterior teeth, creating crowding or retrusion of the maxillary incisors, which deepens the dental overbite but reduces the dental overjet. There is less mandibular dental crowding, but there are impacting third molars. The molar relationship is Class II. The orthodontic classification here is Angle Class II, division 2 malocclusion. (d) AMHypo with agenia leading to mandibular crowding. There is also maxillary crowding and impacted maxillary canines due to a secondary small maxilla. The molars are in a Class I relationship. This would be called Angle Class I malocclusion with severe dental crowding. (e) Severely small maxilla with extreme dental crowding. This is caused by a lack of pneumatization of the maxillary sinuses and is an extension of the state shown in d . Both are caused by open mouth breathing due to the inherent AMHypo. The extreme smallness of the maxilla means the maxillary anterior teeth lie in line with or behind the mandibular anterior teeth, and there is a negative Class III molar relationship. This “malocclusion” gives the illusion that the mandible is too big. The orthodontic classification is Class III malocclusion with severe dental crowding. (f) Here the smallness of the maxilla and the dental crowding are associated with the anterior teeth not meeting at all. This is called anterior open bite , and its genesis pathophysiologically is related to the inherent smallness of the mandible—AMHypo—and is almost always associated with an infantile habit of airway-compensating thumb sucking (see Fig 1-17).
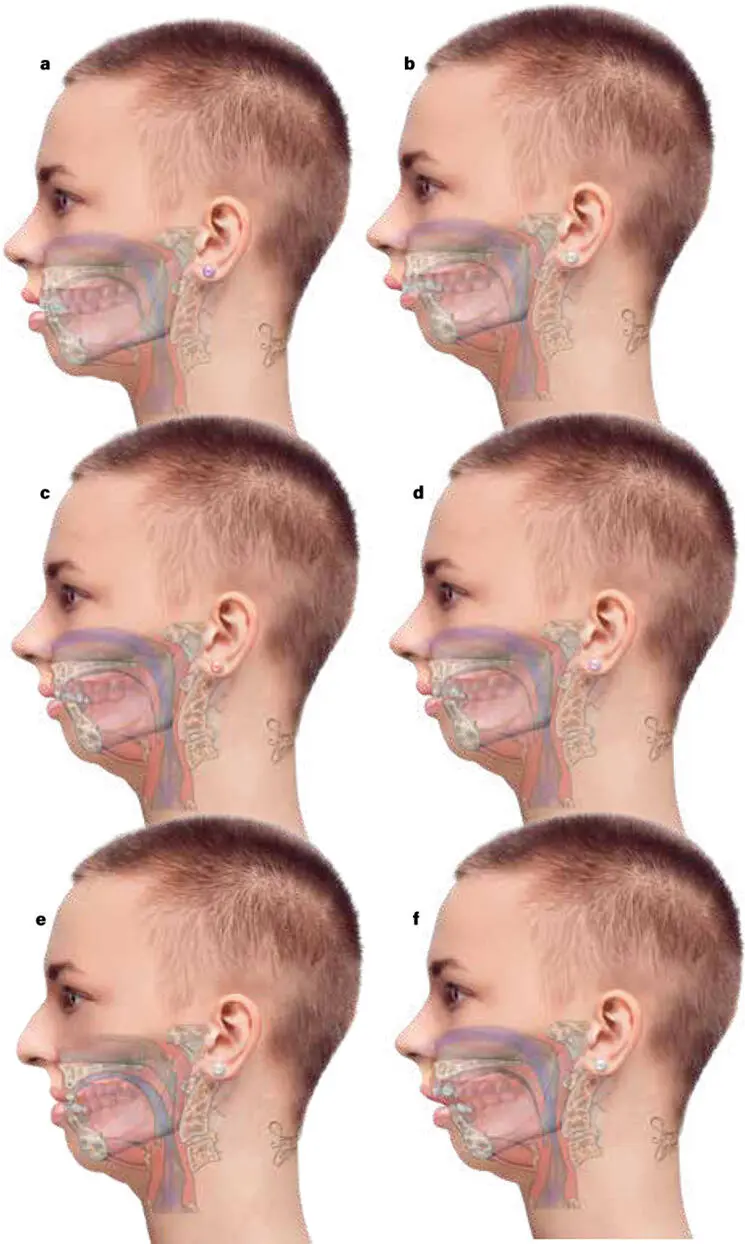
FIG 1-14 Orthognathic malocclusion series 2: Agenia, with and without AMHypo, with and without maxillary hypoplasia, looking at the teeth, tongue, airway, facial profile, and jaw size. By saying that 98% of all malocclusion is caused by AMHypo, our new orthognathic classification can rationalize simultaneously the airway and facial profile effects, in addition to malocclusion of dental crowding patterns. The only additional considerations are therefore (1) Is there a chin? (2) Is there an effect on maxillary development? (3) Is the condylar anatomy normal? (a) Normally proportioned mandible and maxilla without a chin button (agenia). (b) AMHypo with agenia with the maxillary arch drawn normally. (c) AMHypo with agenia with the collapse of the maxillary anterior teeth. (d) AMHypo with agenia leading to mandibular crowding, in addition to a secondary small maxilla leading to maxillary crowding and impacted maxillary canines. (e) Severely small maxilla with extreme dental crowding. Because there is chronic nasal blockage, innate glossoptosis, and agenia (short geniohyoid distance), this state poses the greatest lifetime anatomical risk of OSA. (f) Here the smallness of the anterior maxilla and the dental crowding on a primary base of AMHypo and agenia are associated with the anterior teeth not meeting at all.
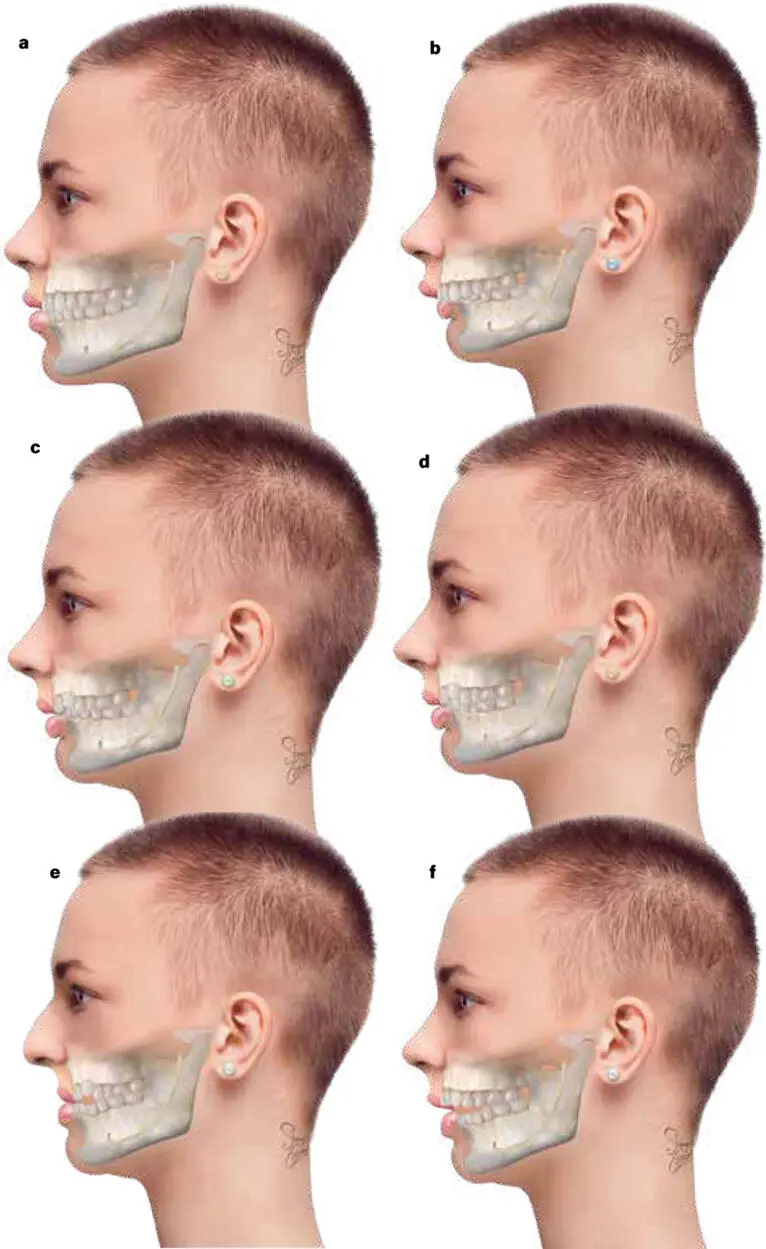
FIG 1-15 Orthognathic malocclusion series 3: Normogenia looking only at the teeth and facial profile and jaw size. (a) Normally proportioned mandible and maxilla with a chin button (normogenia). With a chin button, the lips are closed at rest, and a proportion of the maxillary front teeth are esthetically seen below the line of the relaxed upper lip. The appearance is of a full and complete smile. Orthodontically this would be called Class I normal occlusion without crowding. With a more defined jawline, this is still a very feminine profile but less neotenic (young looking). The geniohyoid is at full stretch, and there is good chin-neck contour. I call this “the California look.” (b) AMHypo with normogenia with the maxillary arch drawn normally. The outward curl of the lips and the slight prominence of the maxillary anterior teeth normalizes nasal projection and nasal-lip balance, and the slight retrusion of the normal chin button is considered in combination very feminine and neotenic. I call this “the soft French look.” (c) AMHypo with normogenia with the collapse of the maxillary anterior teeth. There is relative collapse of the upper lip relative to the base of the nose, giving a sense of overforward nasal size or projection (a common cause to seek cosmetic nasal tip reduction). (d) AMHypo with normogenia leading to mandibular crowding, in addition to maxillary crowding and impacted maxillary canines. There is a prominent lower lip curl because of the collapse of the upper lip. (e) AMHypo with normogenia with a severely small maxilla with extreme dental crowding, leading to buccal crossbite and a high arched palate. The illusion is that the mandible is too big, which is further accentuated by what is essentially still a normal chin button. I call this the “wicked witch of the west” look. (f) Here the smallness of the anterior maxilla and the dental crowding are associated with the anterior teeth not meeting at all. All anterior open bite is associated with infantile glossoptosis, which remains present throughout the lifetime of the individual and is pathologically expressed as OSA in adulthood.
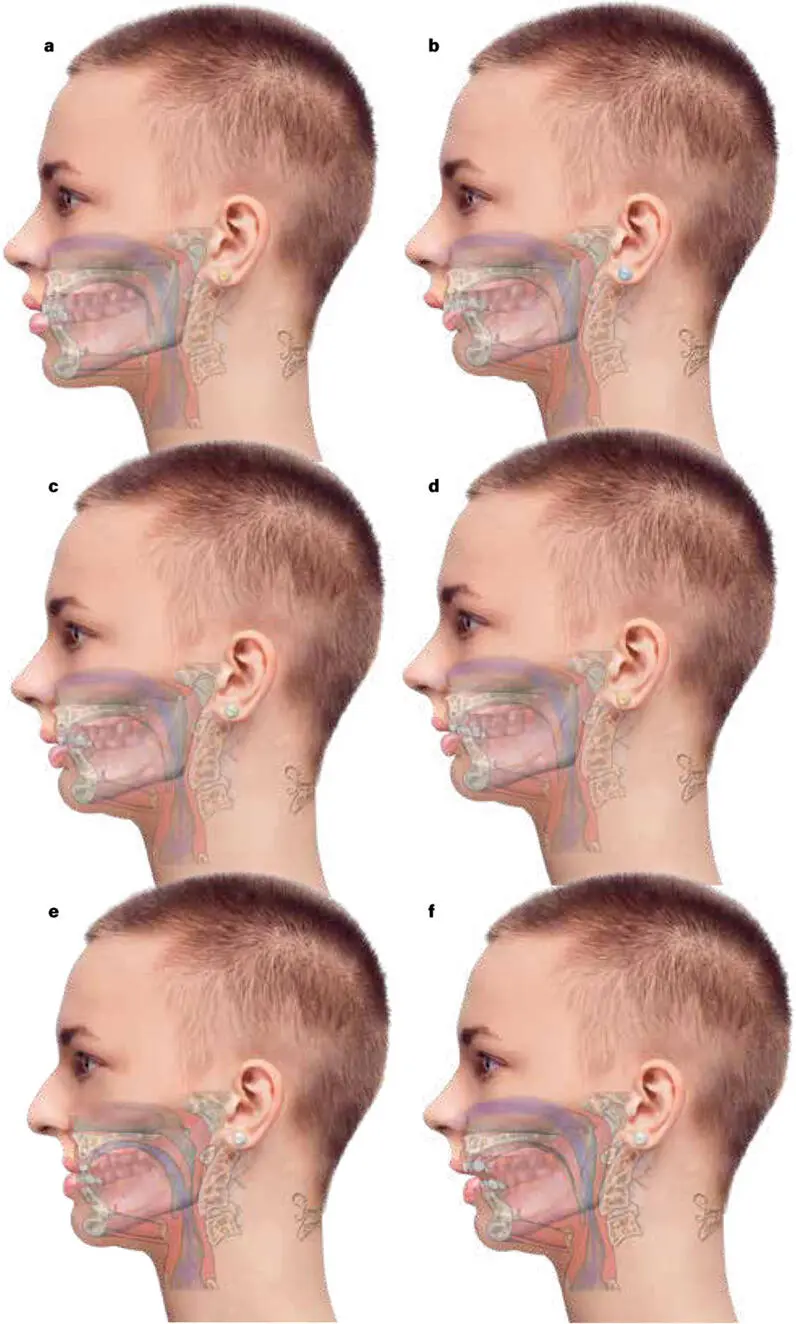
FIG 1-16 Orthognathic malocclusion series 4: Normogenia looking at the teeth, tongue, airway, facial profile, and jaw size. (a) Normally proportioned mandible and maxilla with a chin button (normogenia). This person is at least anatomical risk of lifetime development of OSA. (b) AMHypo with normogenia with the maxillary arch drawn normally. (c) AMHypo with normogenia with the collapse of the maxillary anterior teeth. (d) AMHypo with normogenia leading to mandibular crowding, in addition to maxillary crowding and impacted maxillary canines. (e) AMHypo with normogenia with a severely small maxilla and extreme dental crowding. (f) Here the smallness of the maxilla and the dental crowding are associated with the anterior teeth not meeting at all in anterior open bite. In all these cases (b to f) , the degree of glossoptosis and OSA risk is the same. Assessment of airway state in an erect, toned, and relaxed posture is a different assessment to being supine, relaxed, and in deep sleep, as will be explained in later chapters.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «6Ways to Design a Face»
Представляем Вашему вниманию похожие книги на «6Ways to Design a Face» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.



Обсуждение, отзывы о книге «6Ways to Design a Face» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.