Paul Coceancig - 6Ways to Design a Face
Здесь есть возможность читать онлайн «Paul Coceancig - 6Ways to Design a Face» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:6Ways to Design a Face
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
6Ways to Design a Face: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «6Ways to Design a Face»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
6Ways to Design a Face — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «6Ways to Design a Face», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
CLASS F
Class F describes the presence of AMHypo, with or without a chin button, with normal development of 32 teeth. The third molars may or may not be impacted. Dental crowding is present in the maxilla, but the maxillary anterior teeth only partially overlap, or they openly overlap the line of the mandibular anterior teeth. This condition occurs because of chronic open mouth breathing, where there is over-eruption of the molars, which further props open the front of the mouth, leading to severe lip incompetency. Where the open mouth breathing has been closed because of adaptive thumb sucking in order to drive nasal breathing, there is worsening of the anterior dentoalveolar deformity in the maxilla. Overall the condition may be called “anterior open bite” and is often associated with tongue thrusting (see Fig 1-19), which helps close the oral lip seal and thus enables for normal nasal breathing while awake. Tongue thrusting does not cause the anterior open bite. Anterior open bite is overwhelmingly present only with AMHypo. The association of anterior open bite and glossoptosis is pathognomonic.
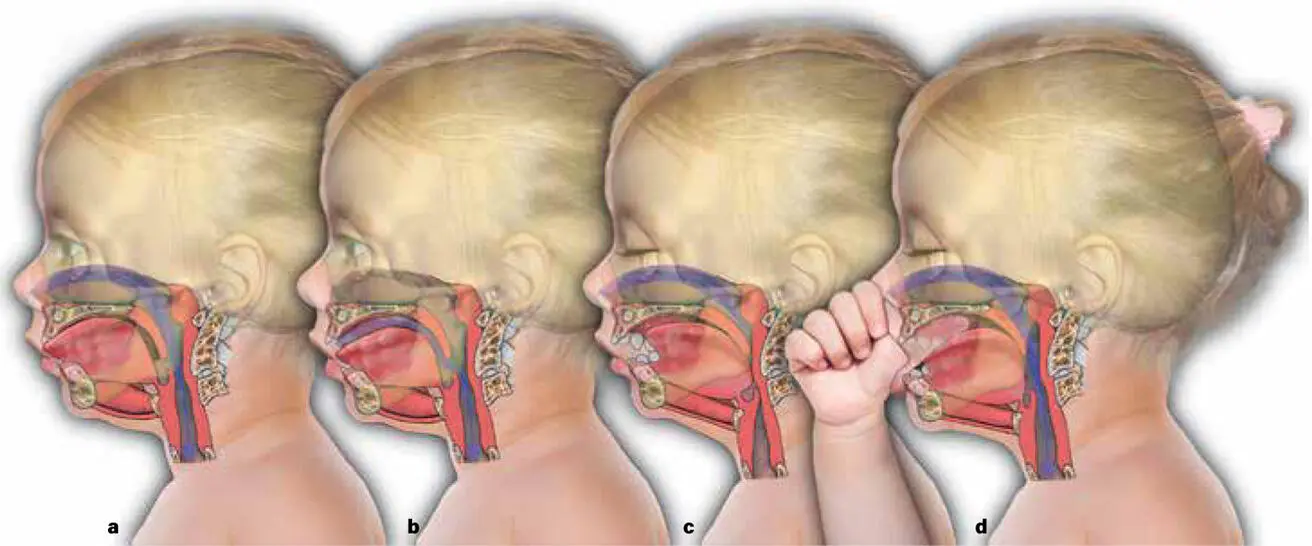
FIG 1-19 A common complaint of orthodontists treating anterior open bite in adolescents is persistent tongue thrusting that they say complicates successful orthodontic therapy. Tongue thrusting (a) as an adaptive position of the tongue has its origin in the infantile period and is only present during the awake state. By closing the hole between the anterior open bite and parted lips, it simultaneously brings the back of the tongue forward and restitutes normal nasal breathing. Tongue thrusting, as with general tongue tone, can only occur during fully awake or light sleep states. Without tongue thrusting, there is no innate oral seal, and obligate open mouth breathing occurs (b) . During deep sleep, with loss of tongue tone and under the influence of gravity with supine sleeping, the relaxed tongue collapses the retroglossal airway completely, which is called glossoptosis (c) . Lying on the side, along with the natural discovery of the thumb, enables the mandible to translate forward and thus opens the retroglossal airway. The second metatarsal joint of the thumb locks behind the incisor teeth, and the lips form a natural seal. The combination enables natural nasal breathing, and a simultaneous natural relief of both oral seal and of glossoptosis (d) . There is nothing unnatural about thumb sucking. Thumb sucking is a naturally adaptive measure to the primary state of AMHypo in order to overcome glossoptosis—and thus survive the neonatal and infantile period. It leads to normal midfacial development and normal sinus health. But it is demonized for the deformation of the anterior maxilla and is blamed as a cause for the development of the small jaw.
ANTERIOR OPEN BITE AND THUMB SUCKING
The adolescent presentation of prominent anterior teeth, a small mandible, tongue thrusting, and anterior open bite malocclusion is seen to be associated with an infant or childhood habit of thumb sucking ( Fig 1-17). How infantile thumb sucking transitions into anterior open bite in the adolescent, and why the infant sucks their thumb in the first place, has been an eternally confused area of clinical philosophy and conjecture involving many craft and interest groups, and thumb sucking is an almost universally demonized childhood habit. In my view, thumb sucking is actually an adaptive response to glossoptosis and a life-saving habit for babies with abnormally small jaws (see Fig 1-19).
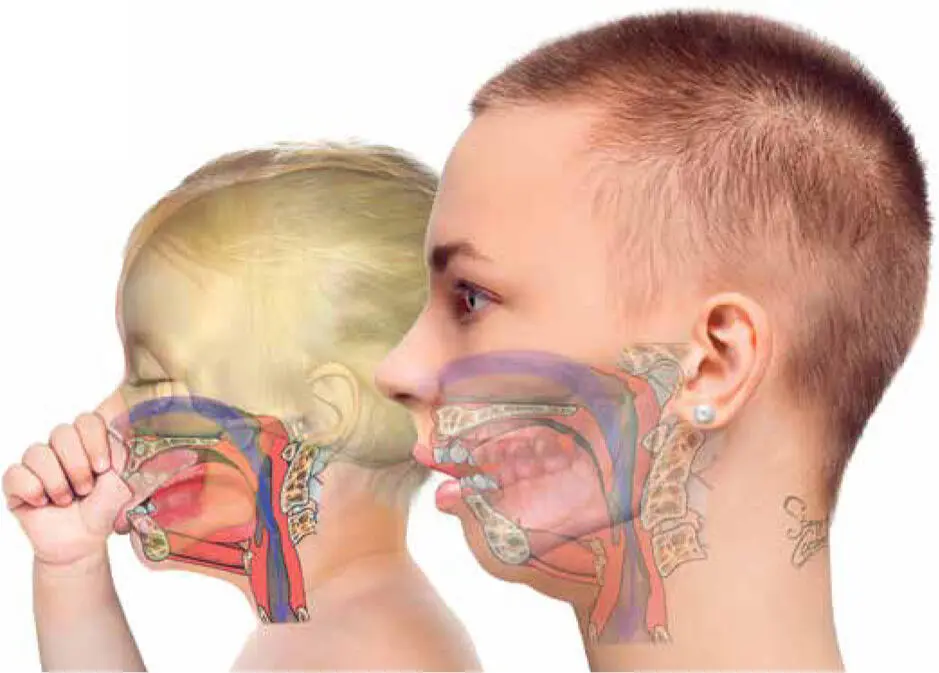
FIG 1-17 Most adolescents and adults with anterior open bite had a thumb sucking habit as an infant or toddler.
To understand anterior open bite is to also understand the interrelationship between concepts of obligate nasal breathing, tongue thrusting, glossoptosis, AMHypo, anterior oral seal, and thumb sucking. Neonates are naturally obligate nasal breathers, and to nasally breathe, the mouth and jaws must be closed and sealed. But in a neonate with a small mandible, and with innate glossoptosis, the baby may find it desperately difficult to nasally breathe while asleep and lying on their back ( Fig 1-18).
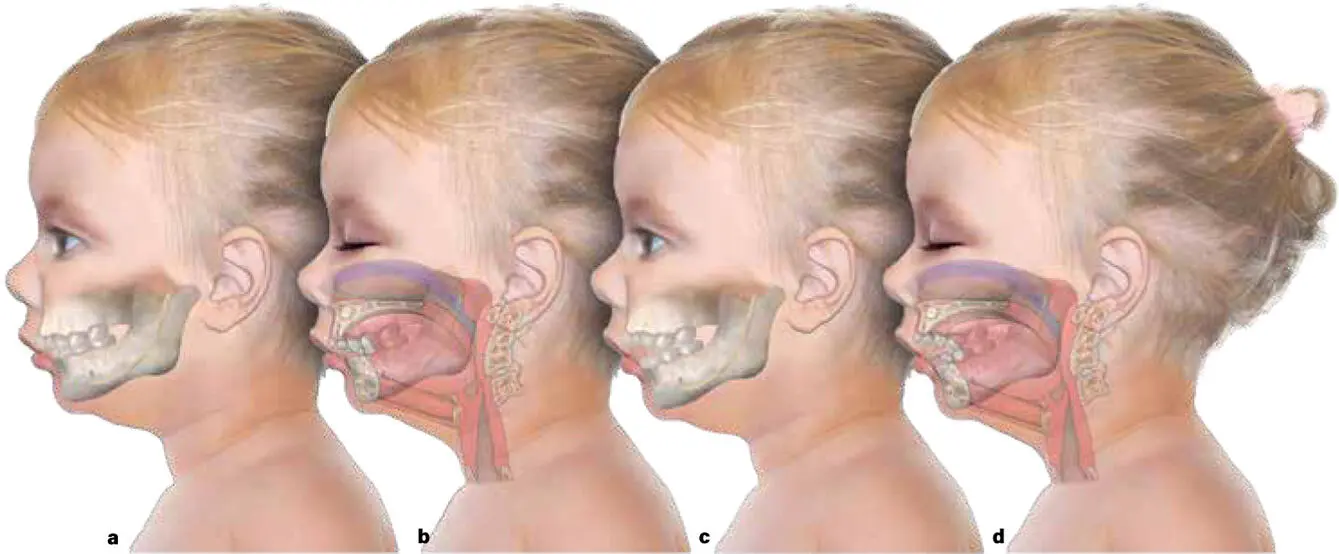
FIG 1-18 A young child with a prominent dental overjet (a and b) and a child with anterior open bite (c and d) have the same inherited small mandible (AMHypo). All that differs between them are the different postural habits that enable them to overcome glossoptosis and nighttime airway collapse. The child with the prominent overjet learns to sleep with their mouth open, lying on their front or side. The child with anterior open bite, on the other hand, learns to suck their thumb to help hold the mandible forward when they sleep in any position. Which way the child randomly selects will lead eventually to an adolescent orthodontic and orthognathic classification.
Pierre Robin was the first person to describe the reasons behind the phenomenon of the “blue baby.” He taught mothers and doctors how to nurse and lay these small-mandible babies prone and on their stomachs to help with breathing. Unfortunately, his insight and knowledge on the dangers of glossoptosis are barely remembered. After all, mothers today are taught to always place their babies on their back to sleep—“back is best” —to reduce the risk of sudden infant death syndrome. But for babies with a small mandible and glossoptosis, there is inherent tongue collapse that blocks normal breathing during supine sleep. Cue the thumb.
A distressed newborn, lying on their back and unable to nasally breathe with a closed mouth, will be reactively unsettled. They will thrash and cry, and the thumb waving in front of them becomes the soother. Not just for comfort like many believe, but because the simple act of sucking the thumb naturally closes the mouth, seals the lips, and holds the tongue and small mandible forward, thereby relieving the glossoptosis and permitting nasal breathing again ( Fig 1-19).
Seen this way, then, thumb sucking is a functional and life-saving adaptation to a fundamentally abnormal anatomical condition. Eventually this thumb sucking becomes a functionally dependent behavior whereby normal nasal breathing, even during supine sleep, becomes possible and dependable and necessary (and terribly hard to break as an unconscious habit later in childhood).
Many dentists and speech pathologists recognize the association between thumb sucking and anterior open bite and small jaws and erroneously assume that the thumb sucking causes the small jaws. But it is actually the other way around. Adolescents and adults with anterior open bite and small jaws have always had an inherently small mandible, and the resulting glossoptosis made it difficult for them to breathe during sleep, hence the natural neonatal survival mechanism of thumb sucking. While almost all people who have anterior open bite sucked their thumbs as children, thumb sucking did not cause their small jaws.
REFERENCE
1.Batista KB, Thiruvenkatachari B, Harrison JE, O’Brien KD. Orthodontic treatment for prominent upper front teeth (Class II malocclusion) in children and adolescents. Cochrane Database Syst Rev 2018;3:CD003452.
2
WHY OBSTRUCTIVE SLEEP APNEA OCCURS
The baby with Pierre Robin syndrome born with a small jaw. The Class II adolescent with braces and impacted third molars ( Fig 2-1). The middle-aged overweight person with sleep-disordered breathing (SDB) and a new diagnosis of obstructive sleep apnea (OSA) supported by a high apnea-hypopnea index (AHI) score. These are all the same person but at different stages of life.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «6Ways to Design a Face»
Представляем Вашему вниманию похожие книги на «6Ways to Design a Face» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.



Обсуждение, отзывы о книге «6Ways to Design a Face» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.