Paul Coceancig - 6Ways to Design a Face
Здесь есть возможность читать онлайн «Paul Coceancig - 6Ways to Design a Face» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:6Ways to Design a Face
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
6Ways to Design a Face: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «6Ways to Design a Face»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
6Ways to Design a Face — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «6Ways to Design a Face», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
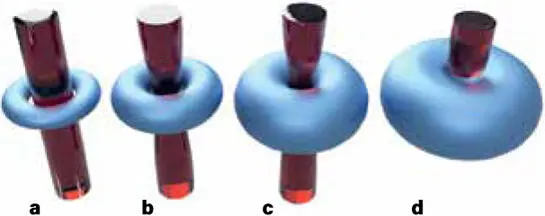
FIG 2-7 A radial neck and inner airway can be teratologically represented and topologically considered as a simple toroid (T). (a) A thin neck has a wide hole and allows for normal laminar noiseless airflow (T > 1). (b) A thickening neck, induced by increasing muscle mass or inner fat, makes the hole smaller (T → 1). The passage of air thins and increasingly becomes turbulent and noisy. Air resistance increases. The venturi of increased inner airflow, particularly with aerobic exercise, induces further collapse. (c) Eventually the neck can be so wide, and the inner airway so small, that we approach a horn torus (T = 1). Increasing airflow pressure through CPAP can overcome this near-complete toroidal collapse, but barely. (d) Once the toroid has collapsed, only increasing air pressure can reliably recreate an already closed airway (0 < T < 1). The greater the toroidal collapse, the more the torus approaches the shape of a sphere (T = 0), where air pressures to regain an airway approaches infinity. Therapeutically creating an incollapsible airway occurs only by making the toroid thinner—through weight loss—or by coring the inner walls through ablative ear, nose, and throat (ENT) surgery; physically stretching the toroid through a MAD; or permanently by advancing the jaw surgically. The toroid provides a physical mathematic model to explain why people become intolerant of CPAP, or are CPAP resistant, where AHI scores do not adequately reduce with CPAP therapy.
Weight control is a huge part of controlling OSA. Fat scans such as dual-energy x-ray absorptiometry (DEXA) can accurately see and monitor fat store loss through diet-selective high-protein, low-carbohydrate ketogenesis. Very low–calorie or food volume–restrictive diets (portion control) can be enhanced by use of intragastric balloons inserted by a gastroenterologist. Weight loss can be more permanently obtained through surgery such as gastric sleeve or gastric bypass procedures performed by an upper GI surgeon.
Surgical treatment of OSA
ENT SURGERY
The common surgical referral given for a person who is unable to control their OSA or snoring—either with CPAP or with a MAD—is ear, nose, and throat (ENT) surgery. ENT surgery traditionally looks at the nasal septum, nasal turbinates, nasal valves, adenoids, tonsils, soft palate, and back of the tongue.
For the nasal septum, the ENT surgeon will resect, carve, and straighten it. This is called a functional septoplasty. ENT surgeons can also open the doorways and remove the walls between the sinuses. This is called fine endoscopic sinus surgery or FESS.
For the turbinates, the ENT surgeon can reduce them. This is called a turbinectomy. For the nasal valves (nostrils), grafts can be placed to widen them. These are called nasal alae, nasal tip lifts, or nostril battens or overall may be called a functional rhinoplasty.
For enlarged or encroaching adenoids behind the soft palate, the ENT surgeon can scrape them away. This is called an adenoidectomy. For enlarged tonsils that seem to fill the back of the mouth behind the tongue, the ENT surgeon can remove them. This is called a tonsillectomy.
For a vibrating soft palate, the ENT surgeon can tighten and scar it using radiofrequencies or surgery and also remove your uvula, especially if it is long. This is called a uvulopalatopharyngoplasty or UPPP. If the back of the tongue is considered too large for the throat, the ENT surgeon can surgically partially remove it. This is called a partial posterior wedge glossectomy.
I place corrective jaw surgery at the top because fundamentally it should correct the absolute “why” behind choking in your sleep in the first place.
The aim of all of these procedures is to reduce the encroachments of the walls and sides and roof and passages of the sinuses, nose, and back of the throat into the airway. In the small rooms and corridors of the upper airways, the ENT surgeon is removing the furniture and inner walls, scouring the paint, and opening the doorways. If, after all this surgery, the patient is still snoring, the ultimate ENT option is to bypass the whole house and create a direct and permanent breathing tube in your trachea. This is called a tracheostomy.
CORRECTIVE JAW SURGERY
At the bottom of the OSA treatment list is corrective jaw surgery, or maxillomandibular advancement (MMA) as ENT surgeons call it. It runs dead last, and it is the only surgical procedure that is not performed by an ENT surgeon. It is also the least understood operation of them all.
For me, and for the reasons I explain in this book, an assessment toward corrective jaw surgery should be at the top of the medical pile. I place it at the top of the list not because it is the best at treating an AHI score. I place it at the top because it is the best at treating everything else that isn’t an AHI score. I place corrective jaw surgery at the top because fundamentally it should correct the absolute “why” behind choking in your sleep in the first place.
THE TRUE CAUSE OF SNORING AND OSA
The fundamental premise of this book is that upper airway obstruction, which leads eventually to apneic episodes during sleep, is caused by a collapsing tongue. This tongue obstruction is called glossoptosis , and it has been a known phenomenon since at least 1923 when it was first described by Pierre Robin in Paris. This tongue collapse occurs more easily when you lie on your back—and during a state of deep sleep—when the body and the tongue lose all tone.
The second fundamental premise of my book is that glossoptosis is inherently associated with people who have small jaws. Small jaws are very common in Western society. Small jaws lead to bad bites and crowded teeth in adolescents, which itself leads to adolescent orthodontic interventions. In older adults, especially as weight is naturally gained, this same small jaw, and the same glossoptosis, inherently leads to a reduced airway lumen, which, promoted by weight gain and the laxity of aging, evolves into the development of snoring and then OSA during deep sleep ( Fig 2-8).
The fundamental premise of this book is that upper airway obstruction, which leads eventually to apneic episodes during sleep, is caused by a collapsing tongue.
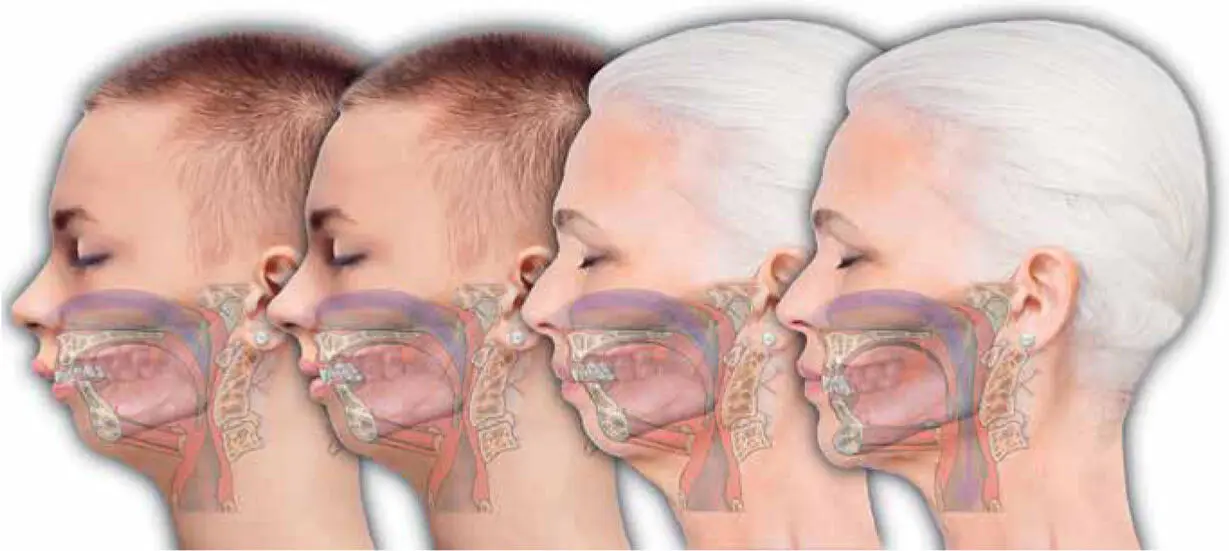
FIG 2-8 Treating the older patient who had camouflage orthodontics as an adolescent through the process of remedial BIMAX is curative for the glossoptosis that is intrinsically linked to the small mandible. Corrective jaw surgery permanently holds the upper airway open (the C3ERPO column) and effectively resists the development of OSA. How that surgical process occurs, and the links that tie all the bits that make up a face together, is explained in the remainder of this book.
The third and most important premise I make is that there is a surgical remedy that can reverse the associated glossoptosis of the small jaw in adolescents as well as correct for the orthodontic consequences of the small jaw. The evolution of this philosophy is to recognize that variants of the same surgical jaw procedures can be used in older people who already have developed OSA in order to cure them of their glossoptosis and therefore reverse their tongue obstruction that is actually causing their OSA.
Remedial corrective jaw surgery
For me, the common reports of adolescent dental crowding, dental extractions, impacted teeth, and orthodontic problems such as a bad bite or prominent anterior teeth in younger years are just as indicative of the reasons underlying why a person has glossoptosis than a standalone consideration of AHI score, CPAP history, diet trials, BMI measure, or medical background. Orthodontics, oral surgery (by way of dental extractions), and ENT procedures (tonsil removal and nasal surgery) are common stories of childhood, and they are also common to many older people who snore or who have OSA.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «6Ways to Design a Face»
Представляем Вашему вниманию похожие книги на «6Ways to Design a Face» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.



Обсуждение, отзывы о книге «6Ways to Design a Face» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.