Atlas of Endoscopic Ultrasonography
Здесь есть возможность читать онлайн «Atlas of Endoscopic Ultrasonography» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Atlas of Endoscopic Ultrasonography
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Atlas of Endoscopic Ultrasonography: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Atlas of Endoscopic Ultrasonography»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Atlas of Endoscopic Ultrasonography Atlas of Endoscopic Ultrasonography, Second Edition
Atlas of Endoscopic Ultrasonography, Second Edition
Atlas of Endoscopic Ultrasonography — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Atlas of Endoscopic Ultrasonography», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
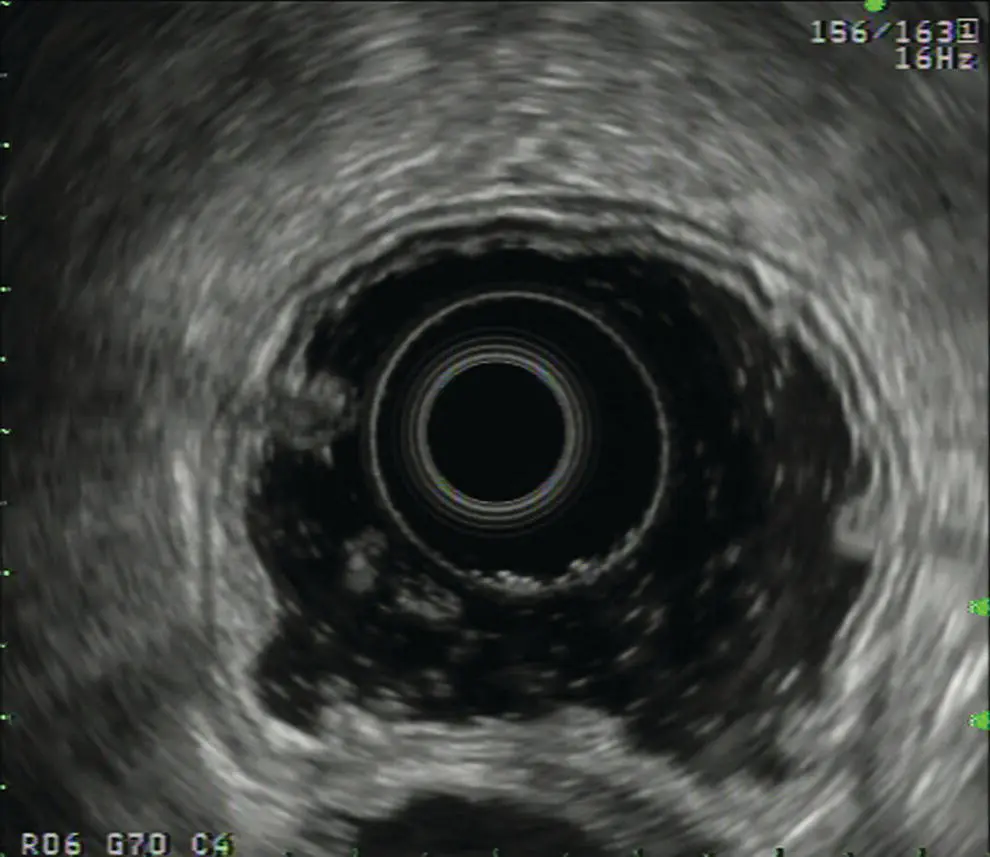
Figure 4.1 Circumferential image of the gastric wall after filling and distending the gastric lumen with water. Image is taken with an electronic radial array echoendoscope at 5 MHz.
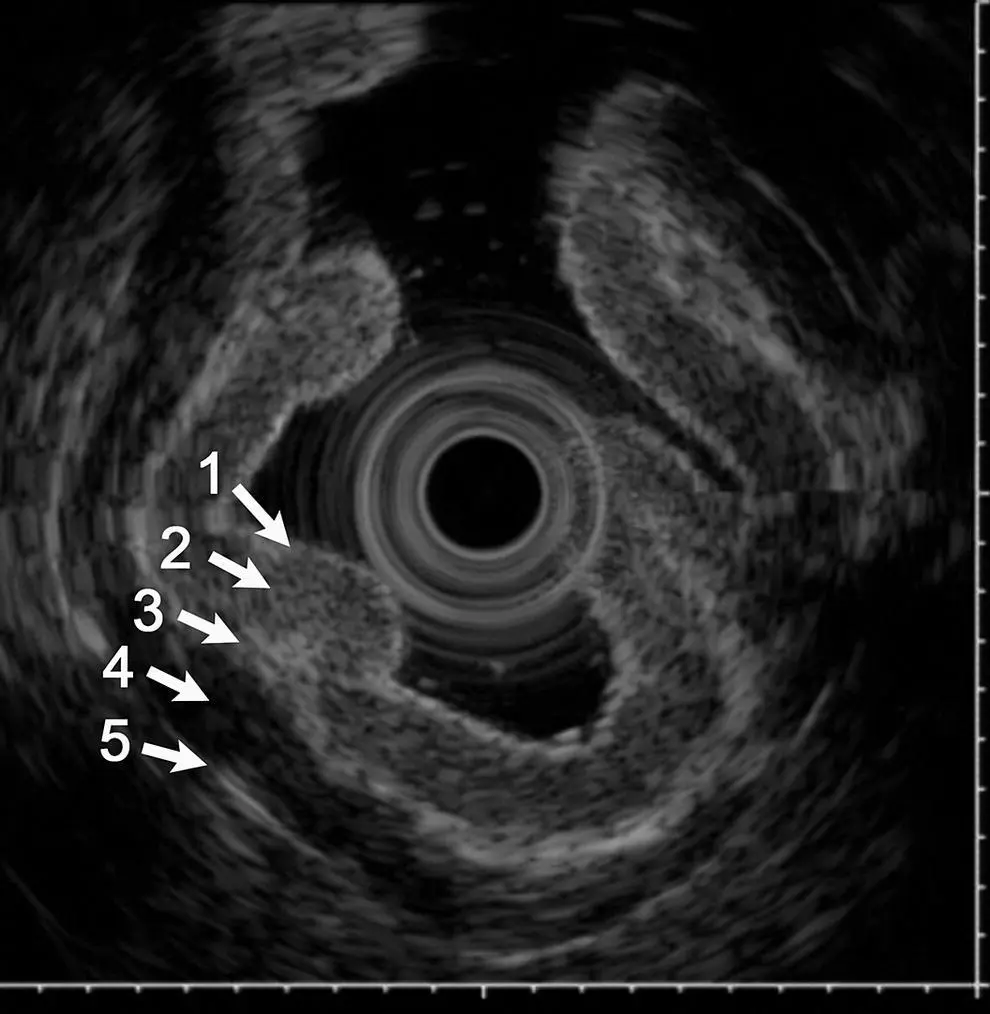
Figure 4.2 Five‐layer structure of the gastric wall demonstrating a relatively thick mucosal layer (layers I and II). Image is taken with a 20 MHz catheter probe.

Figure 4.3 Five‐layer structure of the gastric wall obtained with an electronic radial array echoendoscope at 5 MHz.
1 Interface echo between the superficial mucosa and water (hyperechoic).
2 Deep mucosa (hypoechoic).
3 Submucosa plus the acoustic interface between the submucosa and muscularis propria (hyperechoic).
4 Muscularis propria minus the acoustic interface between the submucosa and muscularis propria (hypoechoic).
5 Serosa and subserosal fat (hyperechoic).
If a high‐frequency (10 MHz or greater) transducer is used, seven or nine layers can potentially be identified on EUS imaging. These nine layers correspond to the following ( Figure 4.4).
1 Epithelial interface (hyperechoic).
2 Epithelium (hypoechoic).
3 Lamina propria plus the acoustic interface between the lamina propria and the muscularis mucosae (hyperechoic).
4 Muscularis mucosae minus the acoustic interface between the lamina propria and muscularis mucosae (hypoechoic).
5 Submucosa plus the acoustic interface between the submucosa and inner muscularis propria (hyperechoic).
6 Inner muscularis propria minus interface between the submucosa and inner muscularis propria (hypoechoic).
7 Fibrous tissue band separating the inner and outer muscularis propria layers (hyperechoic).
8 Outer muscularis propria (hypoechoic).
9 Serosa and subserosal fat (hyperechoic).
An important aspect of EUS imaging in the stomach is to maintain orientation of the imaging plane to avoid tangential imaging, especially when evaluating mucosal lesions. Tangential imaging can result in overstaging of lesions.
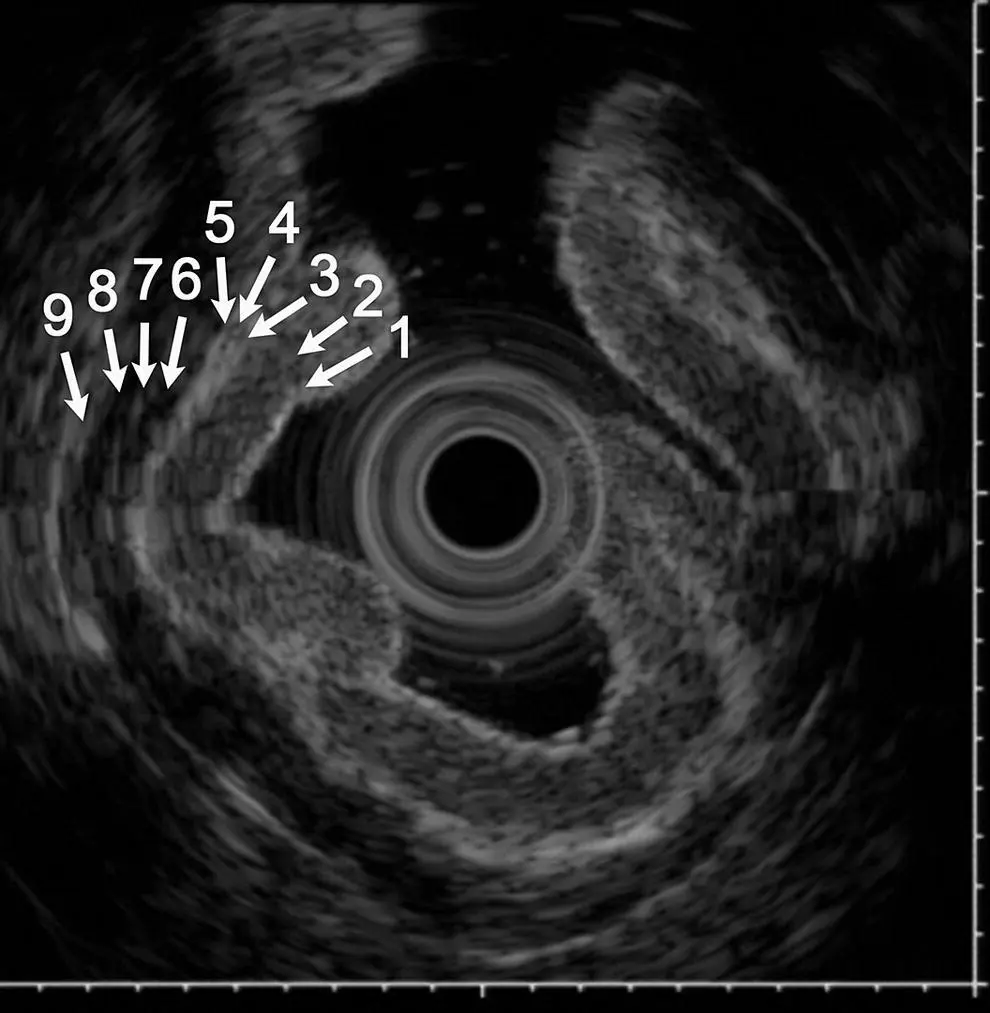
Figure 4.4 Nine‐layer structure of the gastric wall obtained with a 20 MHz catheter probe. The image is the same as Figure 4.2except additional layers are identified.
In conclusion, the only available in vivo method for examining the full thickness of the GI wall, beyond the mucosal surface, is EUS. It provides gastroenterologists with a valuable diagnostic tool to assess pathology in the GI tract to help guide clinical management of the patient. Selection of the correct transducer and using good technique are important in obtaining high‐quality images. When imaging the wall of the GI tract, the method of acoustic coupling is critical. Without good acoustic coupling to the mucosal surface, high‐quality images cannot be obtained. The highest frequency available should be used to image the wall of the GI tract since deep penetration is not necessary unless imaging a large tumor arising from the wall. Using a higher frequency transducer will result in better resolution and allow for better identification of the layers involved. Lower frequencies may be required to identify the size of a mass and if there is involvement with any adjacent structures (T‐staging), and to assess nodal involvement (N‐staging).
Chapter video clip
Video 4.1 Layers of the gastric wall. Source: Aloka.
5 Bile Duct: Radial and Linear
Kapil Gupta
Cedars‐Sinai Medical Center, Los Angeles, CA, USA
Normal bile duct anatomy
Endoscopic ultrasound provides excellent imaging of the biliary tree and gallbladder. Using radial and linear echoendoscope, visualization of the bile duct is performed from two main stations: from the duodenal bulb and from the second portion of the duodenum. The gallbladder is usually seen from the duodenal bulb or the antrum of the stomach. As the entire biliary tree can be visualized only using linear echoendoscope, more endosonographers are primarily using linear echoendoscope for evaluating bile duct anatomy.
Normal anatomy of the bile duct and gallbladder with radial echoendoscope
The echoendoscope is advanced through the pylorus into the duodenal bulb. To achieve this, the scope is usually in a long position along the greater curvature. The big wheel is then turned downwards and the scope is either turned slightly clockwise or the small wheel rotated slightly to the right to deflect the tip of the echoendoscope towards the apex of the duodenal bulb and impacted there. To achieve a stable position the balloon can be inflated, which helps in maintaining the tip of the scope in the bulb.
Here, with slight right and left movement, the liver is oriented at 12 o’clock. In this position the portal vein and the common bile duct can be visualized as two parallel tubular structures to the left of the transducer ( Figure 5.1). With slight right rotation the bile duct can be followed towards the head of the pancreas into the ampulla where a thin pancreatic duct can be visualized below the bile duct ( Figure 5.2). With left rotation or slight counterclockwise rotation the bile duct can be followed upwards into the liver ( Video 5.1).
The gallbladder is usually visualized along the under surface of the liver ( Figure 5.3) and with slight rotation, withdrawing, and pushing the echoendoscope the entire gallbladder can be visualized ( Video 5.1).
To visualize the bile duct from the second portion of the duodenum, the transducer is placed along the ampulla and with slight movement the bile duct and the pancreatic duct can be visualized as two round anechoic structures ( Figure 5.4) ( Video 5.1).
Normal anatomy of the bile duct and gallbladder with linear echoendoscope
The bile duct is visualized with a linear echoendoscope from either the duodenal bulb or the second portion of the duodenum. The transducer of the echoendoscope is advanced across the pylorus. Once in the bulb the balloon can be filled slightly with water to maintain a stable position. Initially the tip of the echoendoscope is impacted at the apex of the bulb; to achieve this, the big wheel is turned downwards. With slightly counterclockwise torque and turning the big wheel down further the bile duct is visualized as a round structure, right in the center of the field ( Figure 5.5). The cut section of the visualized bile duct is in the region of the common bile duct or the common hepatic duct. In this view the portal vein is usually visualized below the bile duct, and also the inferior vena cava (IVC) can be seen to the right of the field ( Figure 5.5). The common hepatic artery can also be visualized coursing in between the bile duct and the portal vein towards the left of the bile duct. From this view the inward impacted position of the tip of the transducer is maintained. By rotating the transducer in a counterclockwise manner the bile duct is followed towards the hilum into the liver and the bifurcation at the porta hepatis can be visualized. Cystic duct take‐off can also be visualized by tracing the bile duct.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Atlas of Endoscopic Ultrasonography»
Представляем Вашему вниманию похожие книги на «Atlas of Endoscopic Ultrasonography» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.




Обсуждение, отзывы о книге «Atlas of Endoscopic Ultrasonography» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.