Atlas of Endoscopic Ultrasonography
Здесь есть возможность читать онлайн «Atlas of Endoscopic Ultrasonography» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Atlas of Endoscopic Ultrasonography
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Atlas of Endoscopic Ultrasonography: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Atlas of Endoscopic Ultrasonography»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Atlas of Endoscopic Ultrasonography Atlas of Endoscopic Ultrasonography, Second Edition
Atlas of Endoscopic Ultrasonography, Second Edition
Atlas of Endoscopic Ultrasonography — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Atlas of Endoscopic Ultrasonography», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
The origin of the celiac artery ( Figure 2.11) is identified and then the scope can be withdrawn. This is the standard reference point for the beginning of the exam during withdrawal. Examination of the extraesophageal and thoracic structures is more time consuming than the radial approach as this echoendoscope’s narrow focal point has to be torqued back a further 180 degrees to cover the same field of examination. This is done by withdrawing the scope at increments with constant back and forth torque.
As the scope is withdrawn 3–5 cm back from the GE junction, the scope will need to be rotated 180 degrees off the aorta to see the left atrium and cardiac structures. The cardiac structure can be discerned quite readily using the linear scope. The mitral valve is just adjacent to the aortic root, which is just at clockwise rotation from the mitral valve. The aortic valve can be visualized at various angles with appropriate endoscopic manipulation given its position relative to the esophagus ( Figure 2.12).
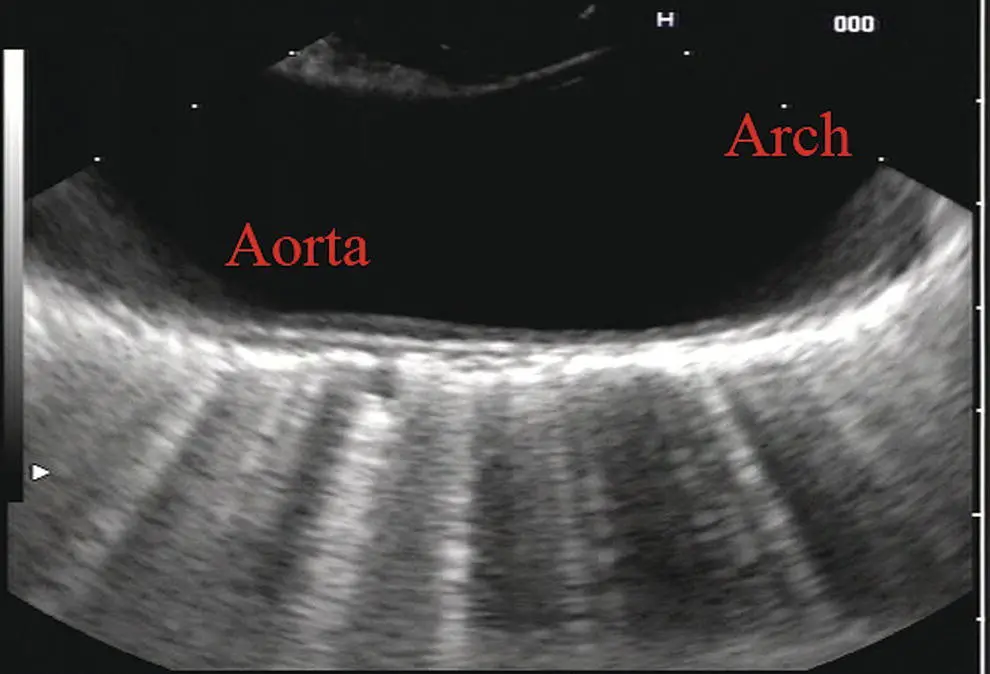
Figure 2.10 Linear array image at the mid aorta.
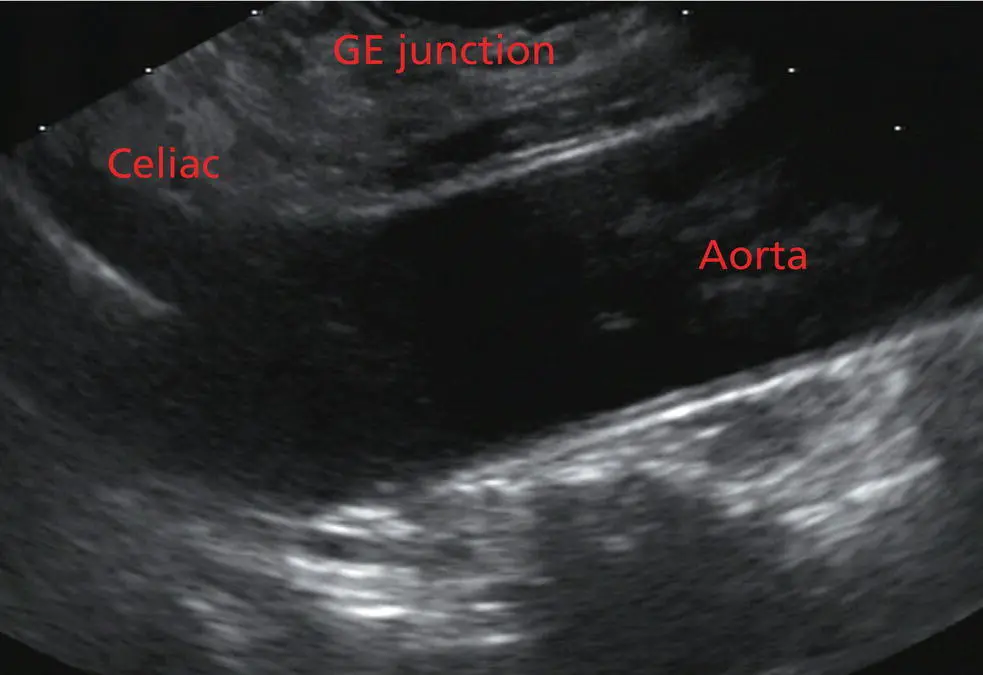
Figure 2.11 Linear array image at the level of the celiac artery.
Withdrawing from the level of the left atrium by 1–2 cm reveals the subcarinal space. This is the area between the pulmonary artery and the left atrium. The bifurcation of the trachea by definition occurs at this level as well.
The AP window is just proximal to this area by several centimeters’ orientation and is slightly clockwise torque from the subcarinal space. The space between the aortic arch and the pulmonary artery make up this region. This is below the level of the aortic arch by a few centimeters. There is a small node seen on the image which could be readily sampled via endoscopic ultrasound‐guided fine needle aspiration (EUS‐FNA) ( Figure 2.13).
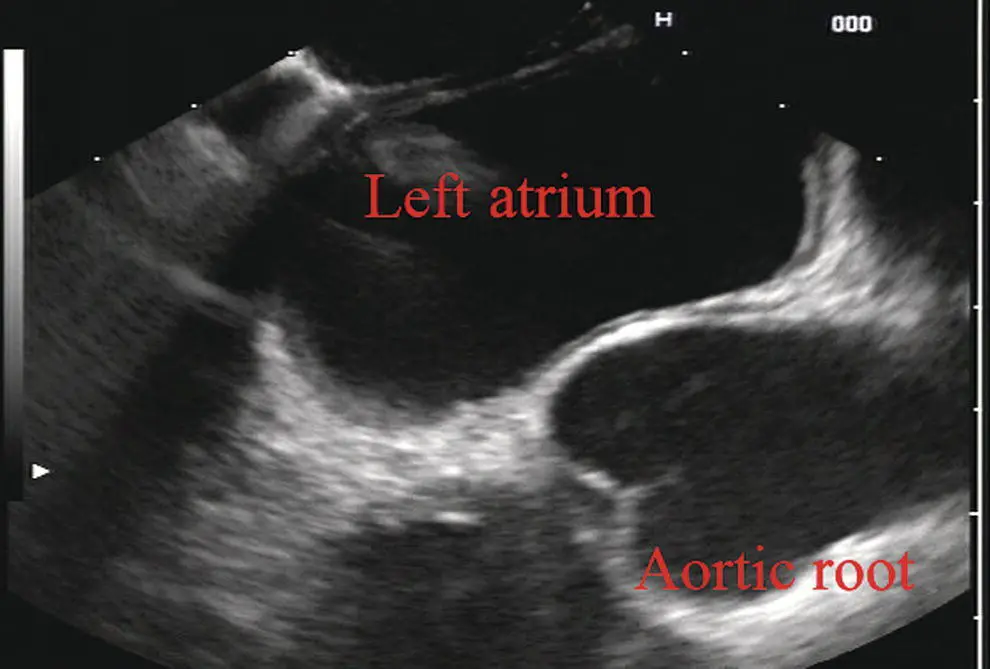
Figure 2.12 Linear array image at the aortic root.

Figure 2.13 Linear array image at the aortopulmonary window (APW). PA, pulmonary artery.
The azygos arch is also visualized around this area, just at or slightly below the aortic arch. The azygos vein can be followed distally along the spine, as in the accompanying Video 2.2. Occasionally intercostal veins are visible.
Chapter video clips
Video 2.1 Radial array examination of the extraesophageal spaces.
Video 2.2 Linear array examination of the extraesophageal spaces.
3 Normal Mediastinal Anatomy by EUS and EBUS
Juan Corral1, Sebastian Fernandez‐Bussy2, and Michael B. Wallace1
1Division of Gastroenterology and Hepatology, Mayo Clinic College of Medicine, Jacksonville, FL, USA
2Division of Pulmonary Medicine and Critical Care, Mayo Clinic College of Medicine, Jacksonville, FL, USA
Introduction
The mediastinum is a common anatomical location for lymph node (LN) metastases in lung cancer as well as many other malignant and inflammatory conditions. The presence and specific location of mediastinal LN metastases in non‐small cell lung cancer (NSCLC) dictates therapy with surgery for localized disease, combination therapy when contralateral LNs are involved, and palliative therapy when contralateral LNs and metastases are encountered. Unfortunately, cross‐sectional imaging with computed tomography (CT), magnetic resonance imaging (MRI), or positron emission tomography (PET) alone is not adequate to confirm a diagnosis; thus, a tissue sample is preferred. Recently, it has been suggested that the use of endoscopic ultrasound‐guided fine needle aspiration (EUS‐FNA) associated with endobronchial ultrasound‐guided transbronchial fine needle aspiration (EBUS‐TBNA) can adequately sample LNs in the mediastinum, avoiding the need for a futile surgery.
The purpose of this chapter is to provide the basic anatomical information as well as technical maneuvers used to investigate the mediastinum successfully.
Anatomical definitions
The LNs in the mediastinum were classified in different stations based on surgical and anatomical landmarks for the purpose of staging lung cancer but this schema is now widely used in other chest diseases ( Figure 3.1). The LNs with their respective stations and corresponding anatomical locations are described in Table 3.1.
EUS‐FNA is usually best suited to sample LNs adjacent to the esophagus which runs posterior to the trachea. Because of ultrasound artifacts created by the air‐filled trachea, lesions immediately anterior to the trachea are not well seen. EUS‐accessible stations include 2L, 2R, 4L, 4R, 5, 7, 8, 9, and, sometimes depending on the size, station 6. On the other hand, EBUS‐TBNA can target LNs either anterior or lateral to the trachea to the level of the carina, and alongside the left and right bronchial tree including stations 2L, 2R, 4L, 4R, 7, 10, and 11. Although both procedures overlap in stations 2 L/R, 4 L/R, and 7, in other stations they are complementary, and in combination allow nearly complete mediastinal access.
Equipment
Radial and curvilinear array echoendoscopes are available ( Figure 3.2), with scanning radius ranging from 270–360 degrees for radial to 100–180 degrees for the linear echoendoscope. These scopes have standard accessory channels (2.0–2.8 mm) and larger accessory channels (3.7 mm) capable of delivering needles and other therapeutic devices such as a 10 French (Fr) plastic stent.
EUS can use several types of needles: 19 gauge (G), 22 G, and 25 G for FNA, as well as Tru‐cut needles for core biopsy. The needle is occluded with a stylet during passage through the gastrointestinal tract wall and bronchial wall to minimize contamination from passage through those structures.
EBUS equipment comprises a curvilinear array echoendoscope with an outer diameter of 6.7 mm and a biopsy channel of 2 mm. The ultrasonic frequency is 7.5 MHz with a penetration depth of 4–5 cm, making it well suited for FNA of LNs and lung masses through the trachea and bronchi. A 22 G needle is used to perform TBNA in the same manner as in EUS. Both systems have integrated oblique‐viewing optics to guide intubation and limited inspection.
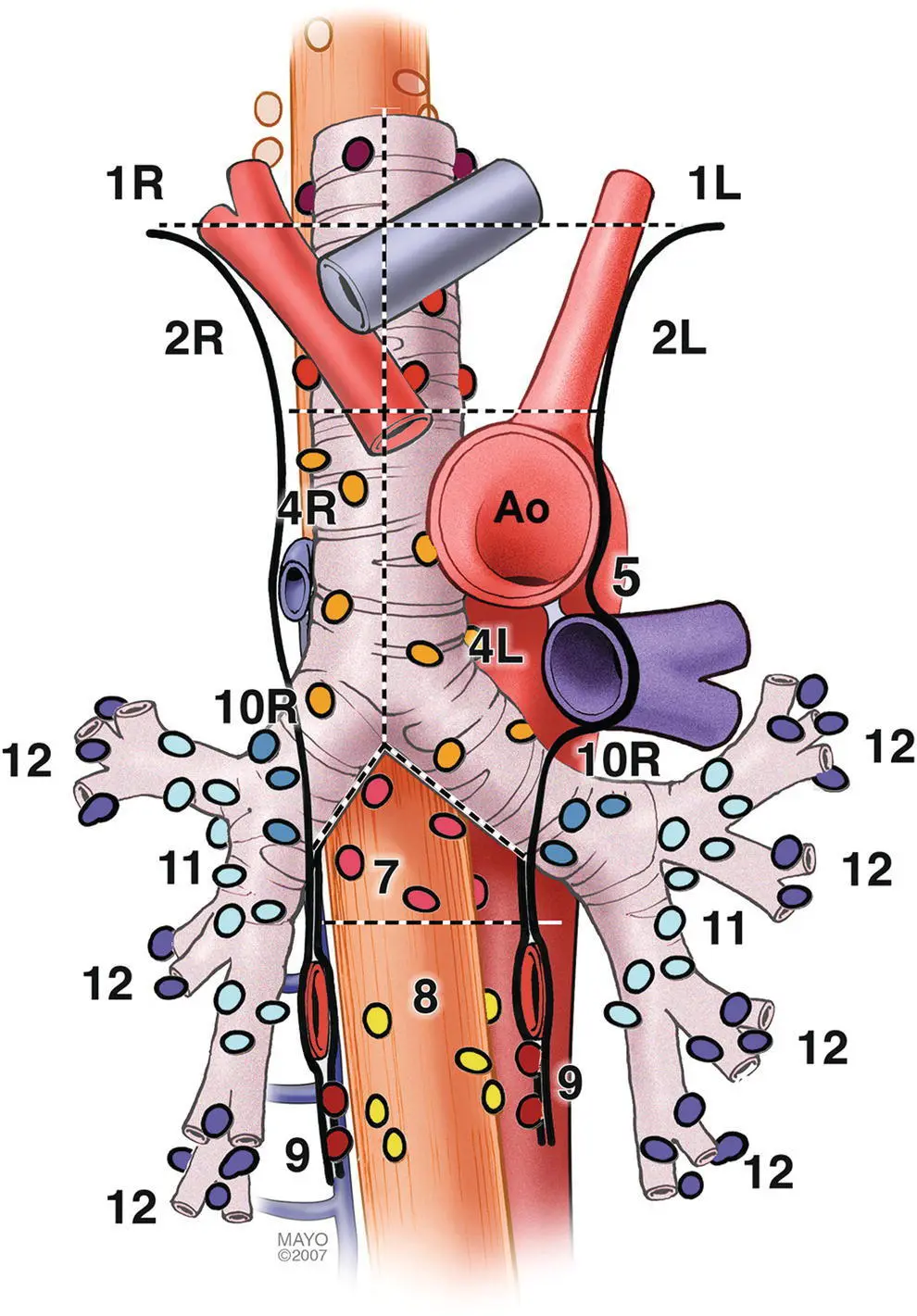
Figure 3.1 Mediastinal lymph node stations.
Endoscopic ultrasound technique
The initial examination can be performed with either the radial or linear array echoendoscope; however, the linear scope is required to perform FNA. Given the obvious efficiencies, we prefer to use a single linear echoendoscope for both imaging and FNA.
Linear scanning
The balloon should be deflated or inflated only slightly to provide good acoustic coupling with the tissue. The mediastinum is imaged by first finding the descending aorta starting at the cardia. The examination can be performed by rotating 360 degrees from the cardia, then withdrawing the shaft 4–5 cm and performing another rotation. Alternatively, one can survey from the cardia to the cervix, then rotating 90 degrees and repeating the maneuver until the whole mediastinum is examined. It is useful to use the following five stations as described by Deprez ( Videos 3.1.1– 3.1.3). For radial examination, see Video 3.2.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Atlas of Endoscopic Ultrasonography»
Представляем Вашему вниманию похожие книги на «Atlas of Endoscopic Ultrasonography» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.




Обсуждение, отзывы о книге «Atlas of Endoscopic Ultrasonography» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.