Stephen J. Bourke - Respiratory Medicine
Здесь есть возможность читать онлайн «Stephen J. Bourke - Respiratory Medicine» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Respiratory Medicine
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Respiratory Medicine: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Respiratory Medicine»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
, a team of distinguished physicians delivers a comprehensive and accessible overview of the essentials of respiratory medicine, including a review of respiratory anatomy and physiology, as well as the aetiology, epidemiology, symptoms, and management of a wide range of respiratory diseases.
This edition offers self-assessment exercises in each chapter and a range of clinical images and scans showing the critical features of each disease. The book also offers:
A thorough introduction to history taking, examination, and investigations Comprehensive explorations of respiratory diseases, including upper respiratory tract infections and influenza, pneumonia, and tuberculosis Practical discussions of bronchiectasis, lung abscess, cystic fibrosis, asthma, and chronic obstructive pulmonary disease In-depth examinations of lung transplantation A companion website featuring figures, key points, and interactive self-assessment questions Perfect for medical students and respiratory nurses,
will also earn a place in the libraries of early-career medical doctors and residents with an interest in respiratory medicine.
Respiratory Medicine — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Respiratory Medicine», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Flow/volume loop
The familiar spirogram plots volume against time (see Fig. 3.2). Forced expiratory manoeuvres may also be displayed by plotting flow against volume. Although the result looks very different, it is worth remembering that it contains precisely the same information. When an inspiratory manoeuvre is also included, the trace returns to its starting point and a flow/volume loop is formed. A normal flow/volume loop is shown in Fig. 3.4.
By convention, the starting point of full inspiration (TLC) is to the left, expiratory flow appears above the horizontal and inspiratory flow is shown below it. At TLC, the airways are at their most stretched (dilated) and airway resistance is minimised, so the maximum (peak) expiratory flow is reached quickly after the start of forced expiration (see Chapter 1). As expiration continues, lung volume progressively diminishes, airway resistance increases and the maximum flow achievable (at each lung volume) declines. In health, this declining portion of the expiratory limb is surprisingly straight. When no further air can be exhaled, flow is zero and the loop reaches the horizontal axis. The inspiratory manoeuvre can then begin. This tends to be more effort‐dependent and therefore less reproducible. Even when perfectly performed, the inspiratory limb is not a mirror image of the expiratory limb. Whilst airway calibre would again favour faster flow nearer TLC, mechanical advantage for the muscles of inspiration means more inspiratory force can be applied nearer residual volume. The coexistence of these two factors produces a more symmetrical inspiratory portion to the loop, with maximum inspiratory flow being at the midpoint of inspiration. Note, too, that maximum inspiratory flow is less than maximum expiratory flow. In forced expiration, the mechanical advantage and airway calibre coincide at the same point in the manoeuvre (the start).
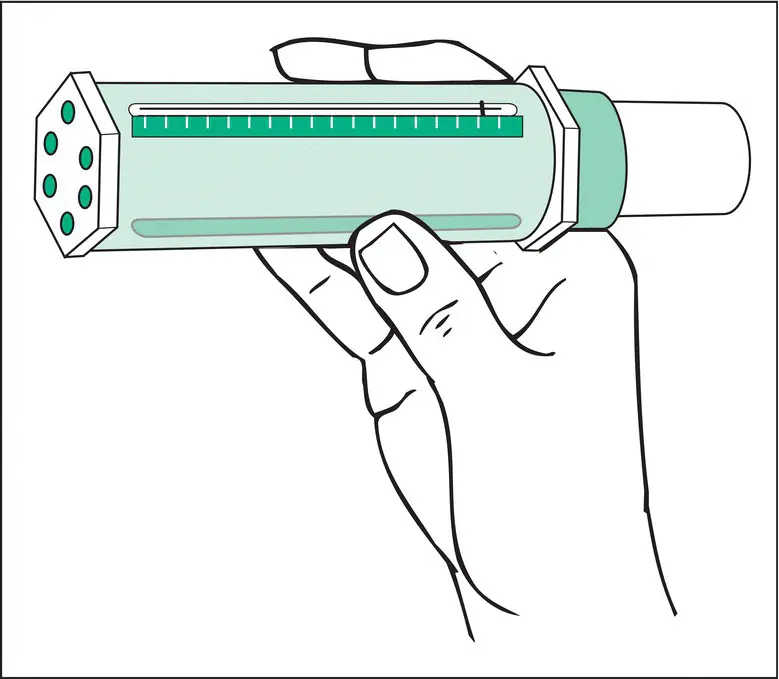
Figure 3.3 Measurement of PEF. The subject takes a full inspiration, applies their lips to the mouthpiece and makes a sudden maximal expiratory blast. A piston is pushed down the inside of the cylinder, progressively exposing a slot in the top, until a position of rest is reached. The position of the piston is indicated by a marker and PEF is read from a scale. It is customary to take the best of three properly performed attempts as the PEF.
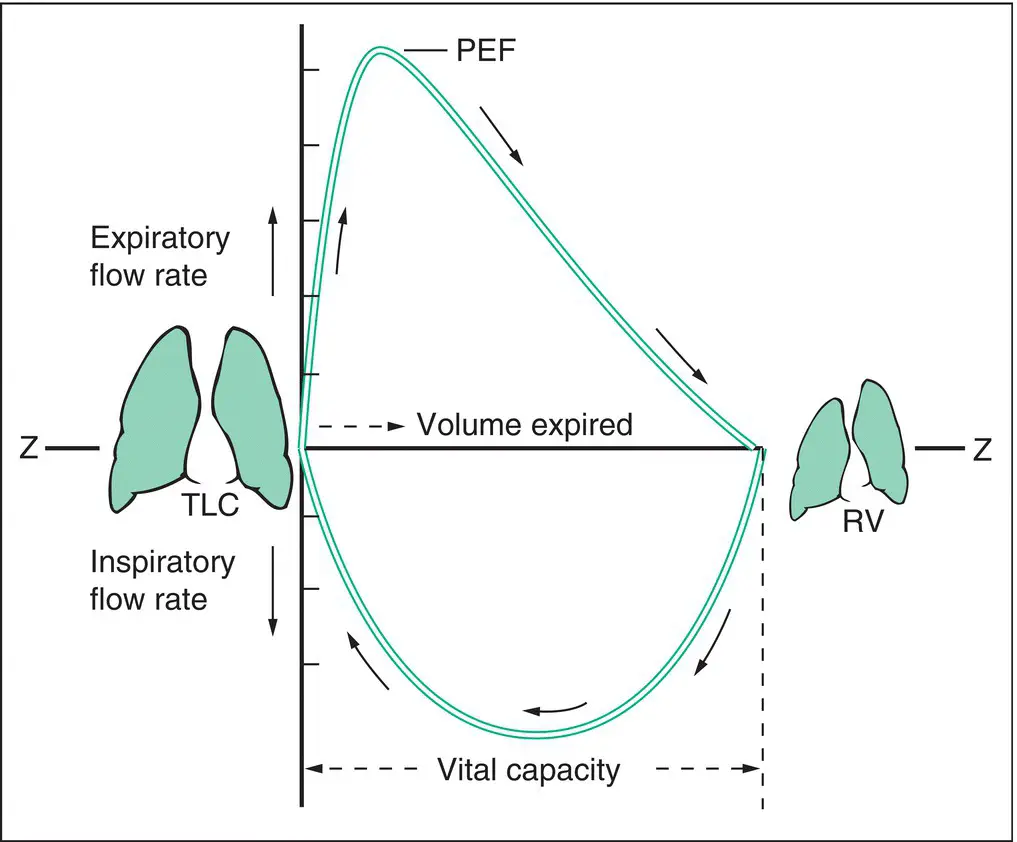
Figure 3.4 Flow/volume loop. Airflow is represented on the vertical axis and lung volume on the horizontal axis. The line Z–Z represents zero flow. Expiratory flow appears above the line; inspiratory flow, below. PEF, peak expiratory flow; RV, residual volume; TLC, total lung capacity.
The flow/volume loop really comes into its own when assessing localised narrowing of the central airways, as illustrated in Figs 3.5and 3.6. Although the traditional spirogram has a characteristic appearance in this context ( Fig. 3.5), the abnormality is not so striking as when observed in the flow/volume loop ( Fig. 3.6d,e). Without the flow/volume loop, large airway obstruction may be overlooked. By comparing the relative effects on the expiratory and inspiratory limbs, it is also possible to determine whether the large airway obstruction is inside (e.g. tracheal stricture) or outside (e.g. compression by a goitre in the neck) the thorax ( Fig. 3.7).
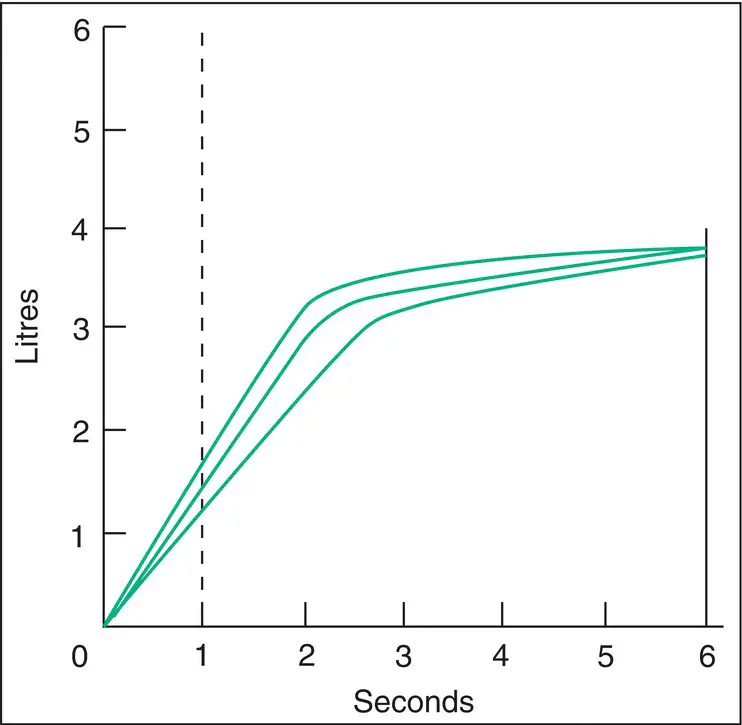
Figure 3.5 Large (central) airway obstruction. Typical tracing obtained with a spirometer. The subject has made three maximal forced expirations. Each shows a striking straight section, which then changes relatively abruptly, at about the same volume, to follow the expected curve of the forced expiratory spirogram. The straight section is not as reproducible as a normal spirogram. A ‘family’ of similar tracings is thus obtained, each with straight and curved sections. Explanation: over the straight section, flow is limited by the fixed intrathoracic localised obstruction. This is little influenced by lung recoil, so the critical flow is similar during expiration and the spirogram appears straight. A lung volume is eventually reached at which maximum flow is even lower than that permitted by the central obstruction. The ordinary forced expiratory spirogram is described after this point. In the example shown, there must be an element of diffuse airway obstruction, as forced expiratory time is somewhat prolonged (see Fig. 3.2c).
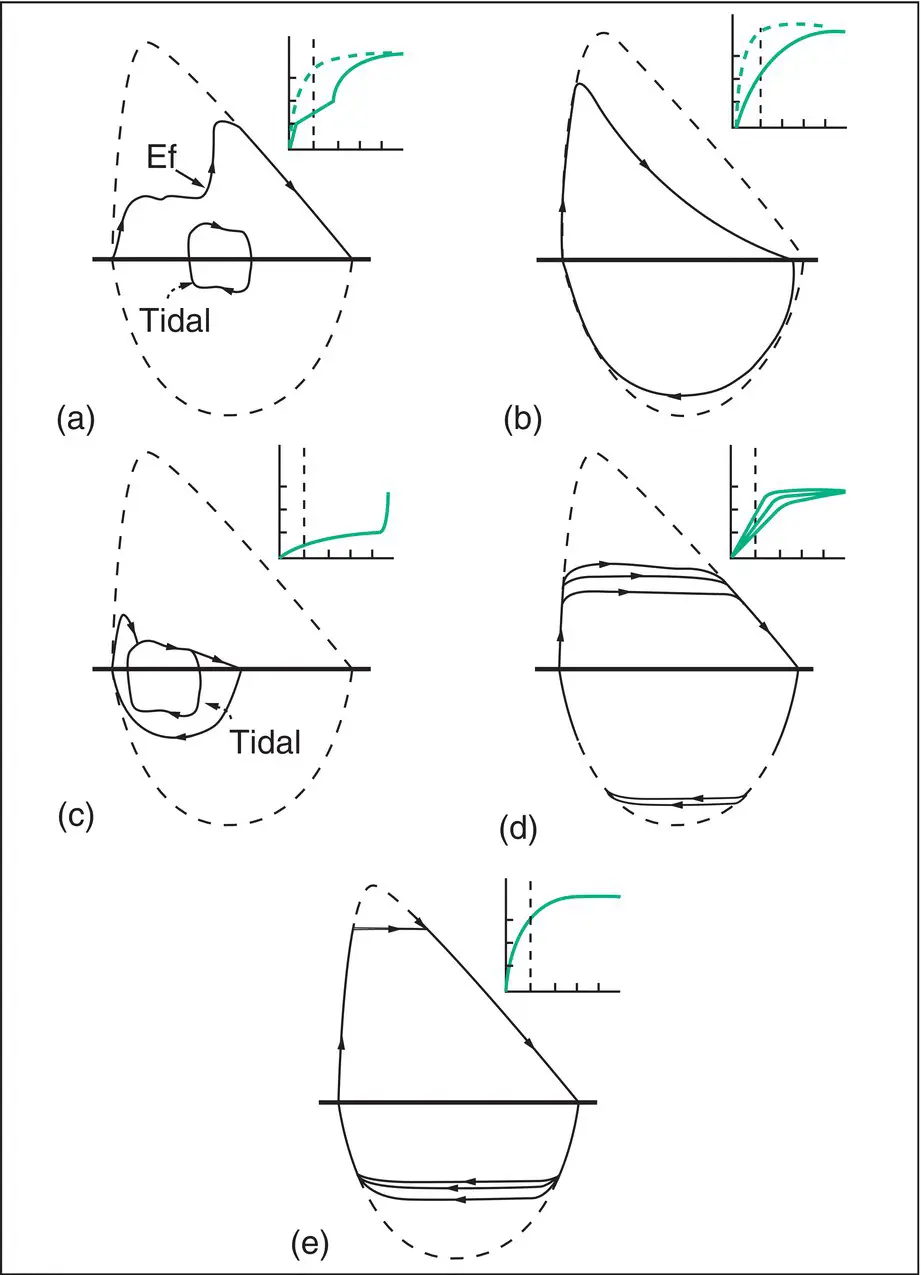
Figure 3.6 Further flow/volume loops. The dotted outline represents a typical normal loop. The small graphs show the appearances of a forced expiration on a spirometer (as in Fig. 3.2). (a) Demonstration of maximum flow. A normal individual makes an unhurried expiration from full inspiration and then, about halfway through the VC, makes a maximal expiratory effort (Ef). The flow/volume tracing rejoins the maximum flow/volume curve, which describes the maximum flow that can be achieved at that lung volume. Also shown is the flow/volume loop of typical tidal breathing. At the resting lung volume, an abundant reserve of both inspiratory and expiratory flow is available. (b) Moderate airway obstruction (asthma or COPD). Maximum expiratory flow is reduced. The declining portion of the expiratory limb has a characteristic curvilinearity. Inspiration is less severely affected. (c) Very severe airway obstruction. Maximum expiratory flow is very severely reduced. There is a brief peak, followed by an abrupt fall in flow rate (probably caused by some airway closure), after which flow falls very slowly. Also shown is a loop representing quiet tidal breathing. It is clear that every expiration is limited by maximum flow. Expiratory wheezing or pursed‐lip breathing would be expected. The tidal loop has been obliged to move to the left, i.e. the patient is ventilating at a higher lung volume. This has obviated, to some degree, the airway narrowing, but adds to the work of breathing and contributes to the sensation of breathlessness (see Chapter 1). (d) Intrathoracic large airway obstruction. Here the peak inspiratory and expiratory flows have been truncated in a characteristic pattern. Intrathoracic lesions (e.g. tracheal compression by a mediastinal tumour) have a more pronounced effect on the expiratory limb than the inspiratory limb. (e) Extrathoracic obstruction (e.g. tracheal compression by a goitre in the neck). This results in inspiratory collapse of the airway below the obstruction (but still outside the thorax), attenuating maximum inspiratory flow rate to a greater degree than maximum expiratory flow rate.
Total lung capacity
The measurement of TLC is not considered in detail here; the interested reader is referred to the reading list at the end of the chapter.
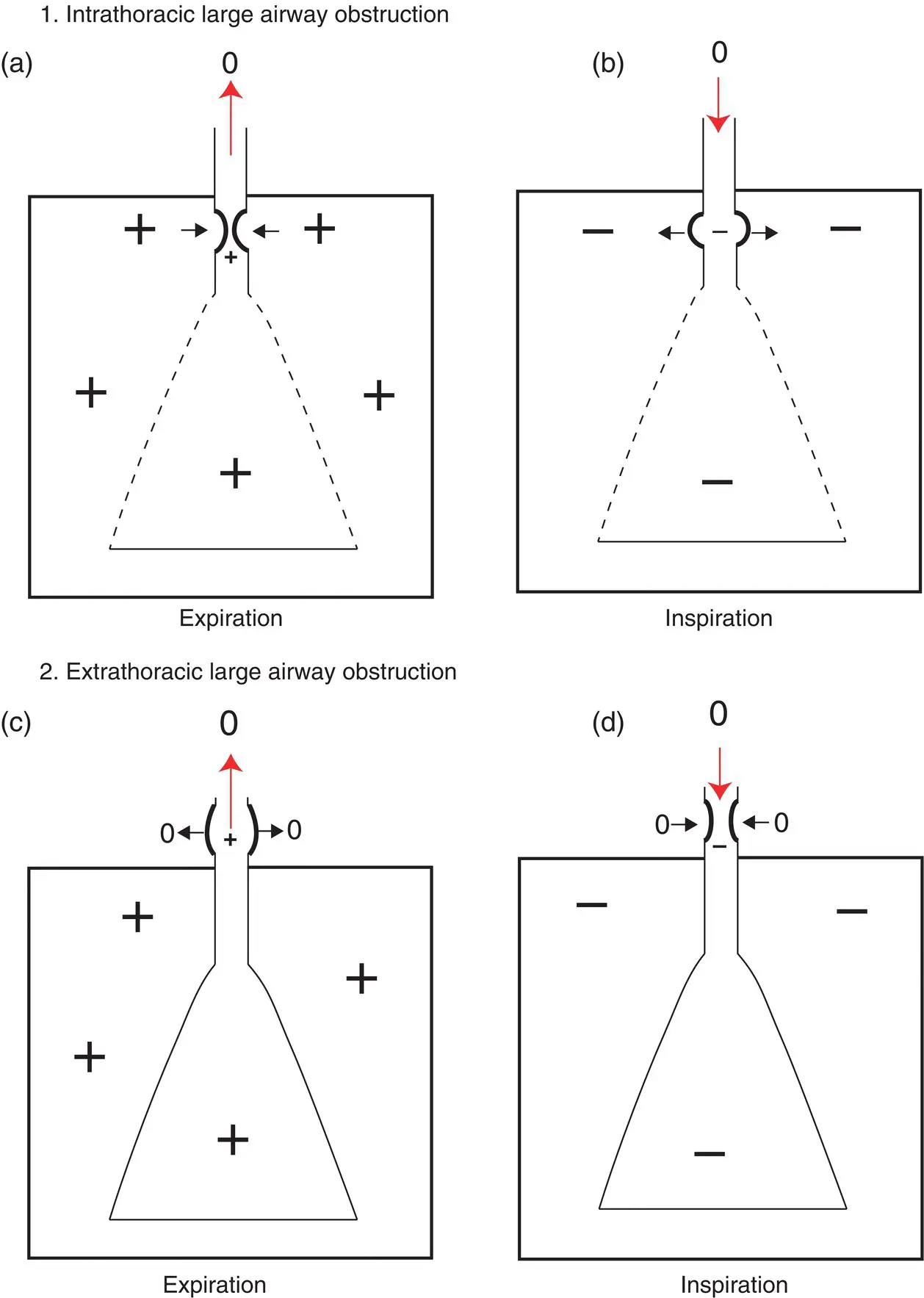
Figure 3.7 Relative effects on expiratory and inspiratory flow of intra‐ and extrathoracic large airway obstruction. Top: Large airway obstruction within the thorax. (a) Positive intrathoracic (alveolar) pressure generated during expiration acts to compress the airway and further narrow the point of obstruction. (b) Negative intrathoracic pressure during inspiration acts to reduce narrowing at the point of obstruction. Therefore, in large airway obstruction within the thorax, expiratory flow is diminished to a greater degree than inspiratory flow (see Fig. 3.6d). Bottom: Large airway obstruction outside the thorax. (c) Positive pressure within the airway during expiration in relation to atmospheric (‘zero’) pressure outside acts to reduce narrowing at the point of obstruction. (d) Negative pressure within the airway during inspiration acts to compress the airway and further narrow the point of obstruction. Therefore, in large airway obstruction outside the thorax, inspiratory flow is diminished to a greater degree than expiratory flow (see Fig. 3.6e).
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Respiratory Medicine»
Представляем Вашему вниманию похожие книги на «Respiratory Medicine» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.






Обсуждение, отзывы о книге «Respiratory Medicine» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.