Stephen J. Bourke - Respiratory Medicine
Здесь есть возможность читать онлайн «Stephen J. Bourke - Respiratory Medicine» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Respiratory Medicine
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Respiratory Medicine: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Respiratory Medicine»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
, a team of distinguished physicians delivers a comprehensive and accessible overview of the essentials of respiratory medicine, including a review of respiratory anatomy and physiology, as well as the aetiology, epidemiology, symptoms, and management of a wide range of respiratory diseases.
This edition offers self-assessment exercises in each chapter and a range of clinical images and scans showing the critical features of each disease. The book also offers:
A thorough introduction to history taking, examination, and investigations Comprehensive explorations of respiratory diseases, including upper respiratory tract infections and influenza, pneumonia, and tuberculosis Practical discussions of bronchiectasis, lung abscess, cystic fibrosis, asthma, and chronic obstructive pulmonary disease In-depth examinations of lung transplantation A companion website featuring figures, key points, and interactive self-assessment questions Perfect for medical students and respiratory nurses,
will also earn a place in the libraries of early-career medical doctors and residents with an interest in respiratory medicine.
Respiratory Medicine — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Respiratory Medicine», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Percussion
Percussion over normal air‐filled lung produces a resonant note, whereas percussion over solid organs, such as the liver or heart, produces a dull note. The percussion note over an area of consolidation is dull; over an effusion, the note is particularly dull (‘ stony dull’). Hyperresonancemay be present in emphysema or over the area of a pneumothorax, although it is rarely a reliable sign. Percussion technique is important and requires practice. The resting finger should be placed flat against the chest wall in an intercostal space (tip: focus on getting the middle phalanx, rather than the whole finger, flat against the chest). The percussing finger should strike the dorsal surface of the middle phalanx and should be lifted clear after each percussion stroke. All areas should be percussed. The order should allow immediate comparison of one area with the equivalent area on the opposite side. To recognise a particular note as hyperresonant takes years of practice and a well‐tuned ear. To pick up a difference between one side and the other is significantly easier. Remember why we have two lungs! When percussing the back of the chest, it is helpful to ask the patient to cross their arms over in front of them, such that one elbow is placed on top of the other. This brings the scapulae forward and out of the way.
Auscultation
Listen with the stethoscope to the intensityand characterof the breath sounds, comparing both sides symmetrically, and note any added sounds(e.g. wheeze, crackles, pleural rub).
Breath sounds
The source of breath sounds in the lungs is turbulent airflow in the larynx and central airways. The quality of the breath sound (as well as the sound of the voice) heard at the chest wall will vary depending on the medium it has to travel through ( Fig. 2.4). A normally aerated lung will conduct low‐pitched sounds modestly but high‐pitched sounds very poorly. Normal breath sounds are therefore rather low‐pitched and faint, and are slightly longer in inspiration than expiration. The rate of airflow at the periphery of the lung is so slow it generates no audible sound at all. Therefore, terms such as ‘good air entry’ and ‘vesicular breath sounds’ are clearly wrong and should be avoided. Normal breath sounds should be called normal breath sounds– it’s that easy.
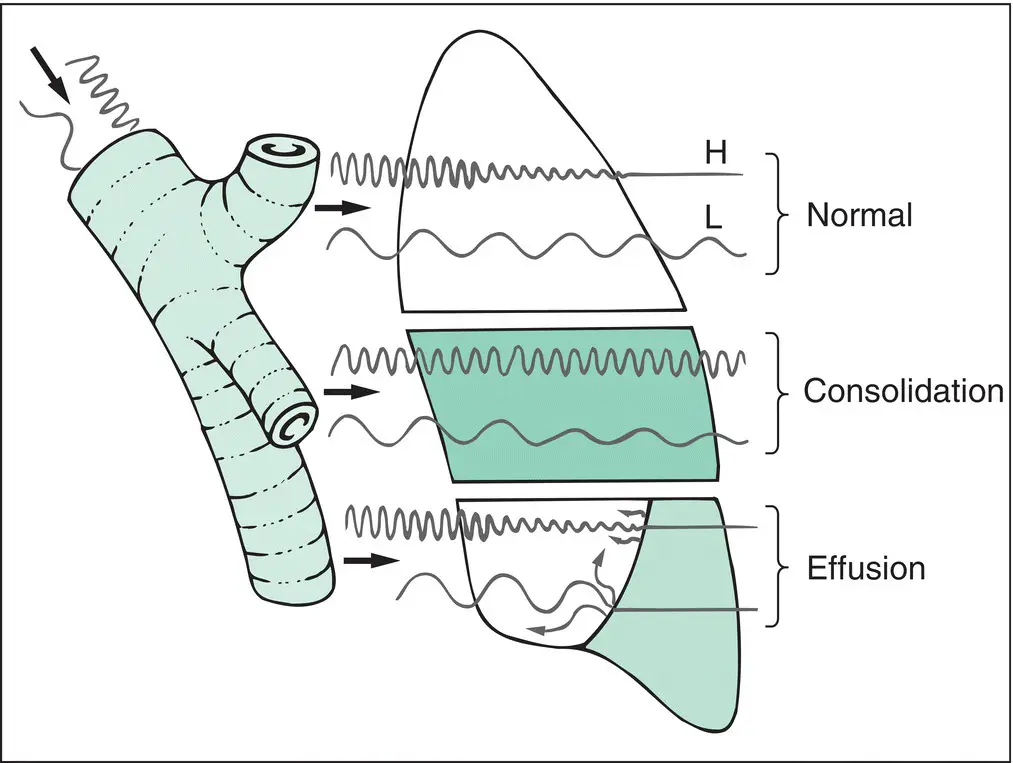
Figure 2.4 Summary of sound transmission in the lung. Sound is generated either by turbulence in the larynx and large airways or by the voice. Both sources are a mixture of high (H)‐ and low (L)‐pitched components. Normal aerated lung filters off the high‐pitched component but transmits the low‐pitched component quite well. This results in soft, low‐pitched breath sounds and low‐pitched vocal resonance. Consolidated lung transmits high‐pitched sound particularly well. This results in loud, high‐pitched breath sounds (bronchial breathing), high‐pitched bleating vocal resonance (aegophony) and easy transmission of whispered (high‐pitched) speech (whispering pectoriloquy). Pleural effusion causes reduction in the transmission of all sound, probably because of reflection of sound waves at the air–fluid interface. Breath sounds are absent and vocal resonance is much reduced or absent.
A solid medium (consolidated lung) conducts sound better, particularly high‐pitched sound. Breath sounds heard over a consolidated lung are therefore similar to those heard with the stethoscope held over the larynx and are referred to as bronchial breathing. The sound is louder and harsher, has a higher frequency ‘hiss’ and tends to be similar in inspiration and expiration.
Vocal resonanceis assessed by listening over the chest with the stethoscope as the patient says ‘ninety‐nine’. Normal aerated lung transmits the ‘booming’ low‐pitched components of speech and attenuates the high frequencies. Consolidated lung, however, transmits the higher frequencies better, so that speech takes on a bleating quality known as aegophony. Whispering ‘ninety‐nine’ produces only high‐pitched sounds. This can barely be heard over normally aerated lung but is transmitted surprising well over consolidated lung and is referred to as whispering pectoriloquy.
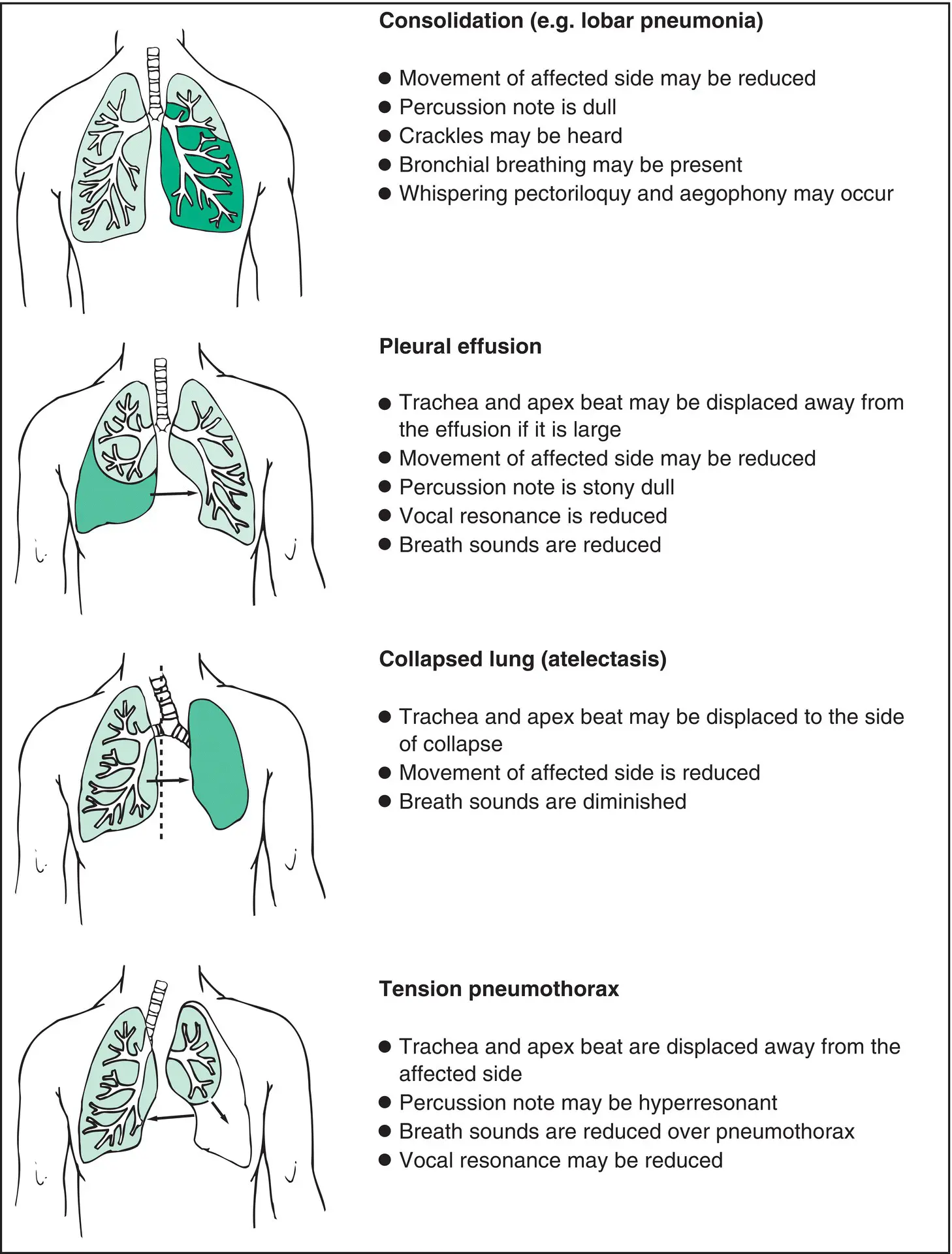
Figure 2.5 Signs of localised lung disease.
A reduction in the intensity of breath sounds ( diminished breath sounds) over an area of lung may indicate obstruction of a large bronchus and collapse of a lobe of the lung. A pleural effusion produces an air–fluid interface, which sound just bounces off. Breath and voice sounds are usually absent over an effusion.
Added sounds
In normal individuals, at auscultation, the inspiratory phaseof respiration seems longer than the expiratory phase. Prolongation of the expiratory phase is a feature of airway obstruction and is often accompanied by wheeze(‘rhonchi’ is redundant and should be avoided): a high‐pitched whistling or sighing sound. Diffuse wheeze is a feature of asthma. Despite the presence of airway obstruction, wheeze is unusual in COPD; diminished breath sounds are more common.
Wheeze localised to one side, or one area of the lung, suggests obstruction of a bronchus by a carcinoma or foreign body (e.g. an inhaled peanut). Remember, inspiratory wheeze is not wheeze, it’s stridor. Stridor indicates the site of obstruction as being in the trachea or main bronchi.
Avoid the term ‘crepitations’ or ‘crepes’ when describing crackles; the existence of two terms only causes confusion. (Most people have a clear idea of the difference in meaning between the two terms; unfortunately, everyone’s idea is different.) Language should facilitate communication, so keep it simple. If the crackles are coarse, they should be described as coarse crackles; if they are fine, they should be called fine crackles. (Reserve the term ‘crepes’ for those thin pancakes you get in France.) It is thought that crackles are produced by the opening of previously closed bronchioles. Early inspiratory cracklesare sometimes heard in patients with a little excess airway mucus (e.g. COPD), but these may diminish or even disappear when the patient is asked to cough. Late inspiratory cracklescan sometimes be heard at the lung bases in obese individuals as the poorly ventilated areas open at the end of a deep breath. Paninspiratory cracklescan be fine (like Velcro), representing lung fibrosis or pulmonary oedema. Coarse paninspiratory crackles usually imply excess purulent airway secretions, as seen in bronchiectasis. Remember: distinguishing coarse from fine is much easier if you remembered to ask the patient to cough at the start of the examination.
Pleural rubsare ‘creaking’ sounds. They are often quite localised and indicate roughening of the normally slippery pleural surfaces. They are heard in the context of pleural inflammation due to either infection or infarction (pulmonary embolism).
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Respiratory Medicine»
Представляем Вашему вниманию похожие книги на «Respiratory Medicine» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.






Обсуждение, отзывы о книге «Respiratory Medicine» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.