Stephen J. Bourke - Respiratory Medicine
Здесь есть возможность читать онлайн «Stephen J. Bourke - Respiratory Medicine» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Respiratory Medicine
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Respiratory Medicine: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Respiratory Medicine»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
, a team of distinguished physicians delivers a comprehensive and accessible overview of the essentials of respiratory medicine, including a review of respiratory anatomy and physiology, as well as the aetiology, epidemiology, symptoms, and management of a wide range of respiratory diseases.
This edition offers self-assessment exercises in each chapter and a range of clinical images and scans showing the critical features of each disease. The book also offers:
A thorough introduction to history taking, examination, and investigations Comprehensive explorations of respiratory diseases, including upper respiratory tract infections and influenza, pneumonia, and tuberculosis Practical discussions of bronchiectasis, lung abscess, cystic fibrosis, asthma, and chronic obstructive pulmonary disease In-depth examinations of lung transplantation A companion website featuring figures, key points, and interactive self-assessment questions Perfect for medical students and respiratory nurses,
will also earn a place in the libraries of early-career medical doctors and residents with an interest in respiratory medicine.
Respiratory Medicine — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Respiratory Medicine», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Respiratory alkalosis (cases are usually acute, as the causes are rarely sustained): pH raised, PCO2 reduced, bicarbonate normal
Alveolar hyperventilation causes a fall in PCO 2and a corresponding rise in pH. Bicarbonate concentration is virtually unchanged. This pattern is seen in any form of acute hyperventilation, including pulmonary embolism, acute severe asthma, anxiety‐related hyperventilation, salicylate poisoning and Covid‐19 pneumonia.
Metabolic acidosis: pH reduced, PCO2 reduced, bicarbonate reduced
The primary disturbance is generally an increase in acid. This has an effect on the equation
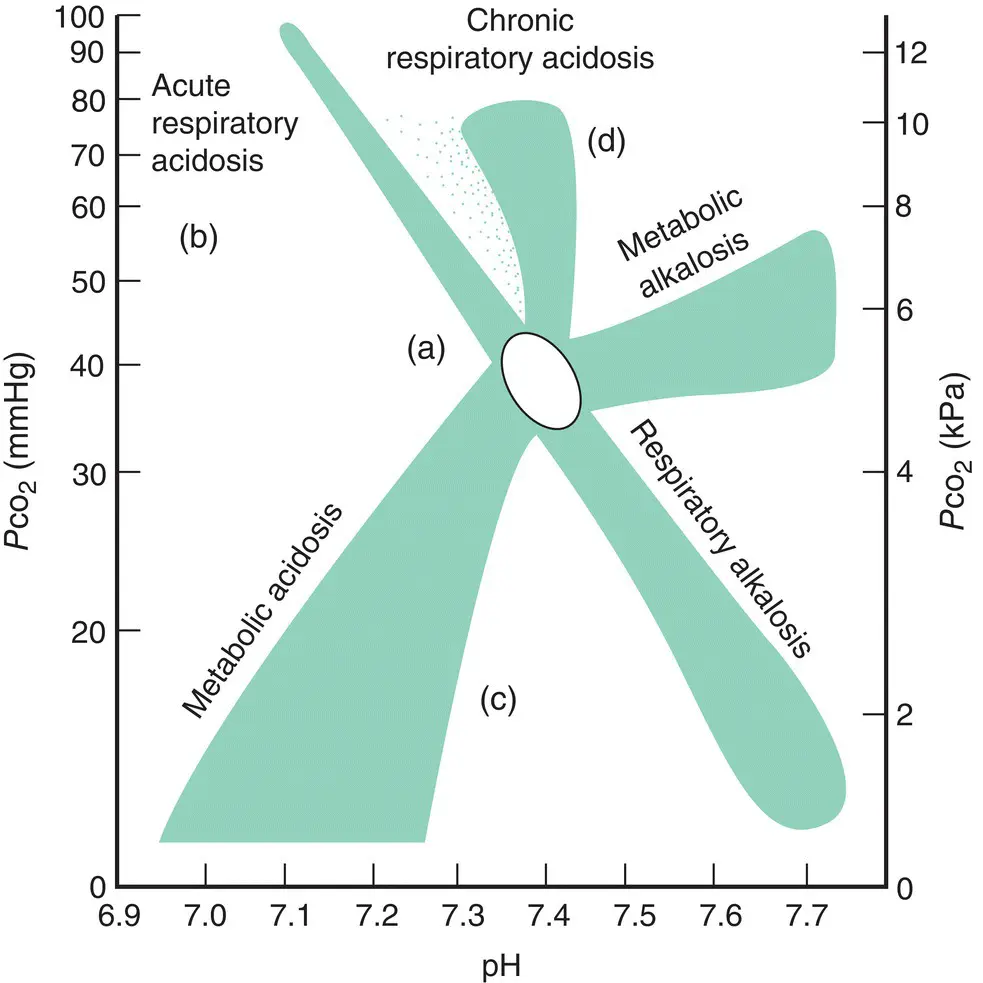
Figure 3.10 Acid/base disturbances. The oval indicates the normal position, the shaded areas indicate the directions of observed ‘pure’ or uncomplicated disturbances of acid/base balance. Bicarbonate levels are omitted for clarity. Letters (a)–(d) are referred to in the section on mixed disturbances.
H ++ HCO 3 −⇌ H 2O + CO 2, pushing it to the right. The CO 2produced is removed by increased ventilation and the net result is a lowering of plasma bicarbonate. In practice, the fall in pH causes further respiratory stimulation, so that CO 2is promptly blown off, and the pH changes are therefore much less dramatic than they would have been. The arterial point moves in the direction indicated in Fig. 3.10. This respiratory compensation is an inevitable accompaniment of metabolic acidosis – acute and chronic – unless there is some other factor limiting ventilatory function or responsiveness.
This pattern is seen in diabetic ketoacidosis, renal tubular acidosis, acute circulatory failure, sepsis and other forms of lactic acidosis.
Metabolic alkalosis: pH raised, PCO2 high normal or slightly raised, bicarbonate raised
An increase in bicarbonate concentration causes a rise in pH. To compensate, ventilation is reduced in order to accumulate CO 2. This occurs despite the inevitable fall in PO 2. For this reason, however, scope for correction is limited; the compensatory fall in alveolar ventilation is modest and correction in pH may not be complete.
This pattern is seen where there has been administration of excessive alkali, loss of acid through vomiting or reabsorption of bicarbonate (e.g. in hypokalaemia).
Mixed disturbances
Mixed respiratory and metabolic disturbances are common. There are usually a number of possible explanations, so it is essential to consider all the clinical details before interpreting the acid/base data. Fig. 3.10shows the situations that may arise in complex acid/base disturbances.
Fig. 3.10a (low pH, normal PCO2, low bicarbonate) indicates a mixed metabolic and respiratory acidosis. The metabolic disturbance is perhaps obvious and the respiratory component can be deduced, as the PCO2 is higher than might have been suspected had this been a pure metabolic problem. This pattern could arise in a number of different clinical scenarios, such as a patient with acute severe pulmonary oedema with low cardiac output and ventilatory compromise or a patient in renal failure given a narcotic sedative suppressing ventilatory response to acidosis. Blood gas results should be interpreted in light of clinical data.
Fig. 3.10b could represent the situation soon after a cardiac arrest, where severe lactic acidosis exists and ventilation has been insufficient.
Fig. 3.10c could represent the situation in severe aspirin poisoning, where aspirin‐induced hyperventilation has been complicated by aspirin‐induced metabolic acidosis.
Fig. 3.10d could represent the situation in an individual with chronic ventilatory failure as a result of COPD who is stimulated to increase ventilation by a pulmonary embolism.
Arterial oxygenation
In addition to the acid/base balance, arterial blood gas analysis provides valuable information on arterial oxygen tension (P aO 2).
Respiratory failure
‘Respiratory failure’ is a clinical term used to describe a failure to maintain oxygenation (usually taken as an arbitrary cut‐off point of PO 28.0 kPa [60 mmHg]).
Type I respiratory failure is hypoxaemia in the absence of hypercapnia. Overall alveolar ventilation is therefore normal. This pattern of abnormality usually indicates a disturbance of the V/Q matching system within the lung. Such a disturbance can be caused by any intrinsic lung disease affecting the airways, parenchyma or vasculature (e.g. acute asthma, lung fibrosis or pulmonary embolism).
Type II respiratory failure is hypoxaemia with hypercapnia and indicates alveolar hypoventilation. Note this is not merely a severe form of type I respiratory failure; it is brought about by an entirely different mechanism. This may occur from reduced ventilatory drive (e.g. sedative overdose), reduced neuromuscular power (e.g. myopathy) or resetting of the chemoreceptors that drive ventilation in chronic lung disease (e.g. COPD).
Of course, type I and type II respiratory failure can coexist (and commonly do). These matters are dealt with in more detail in Chapter 1.
Oxygen saturationcan be measured non‐invasively and continuously using a pulse oximeter. Oxygenated blood appears red, whereas reduced blood appears blue (clinical sign of cyanosis). An oximeter measures the ratio of oxygenated to total haemoglobin in arterial blood using a probe placed on a finger or earlobe, which comprises two light‐emitting diodes – one red and one infrared – and a detector. The light absorbed varies with each pulse, and measurement of light absorption at two points on the pulse wave allows the oxygen saturation of arterial blood to be determined. The accuracy of measurement is reduced if there is reduced arterial pulsation (e.g. low‐output cardiac states) or increased venous pulsation (e.g. tricuspid regurgitation, venous congestion). Skin pigmentation or the use of nail varnish may interfere with light transmission. Oximetry is also inaccurate in the presence of carboxyhaemoglobin (e.g. in carbon monoxide poisoning), which the oximeter detects as oxyhaemoglobin.
The relationship of PO 2to oxygen saturation is described by the oxyhaemoglobin dissociation curve(see Fig . 1.9). This curve is sigma‐shaped, so that oxygen saturation is closely related to PO 2only over a short range of about 3–7 kPa. Above this level, the dissociation curve begins to plateau and there is only a small increase in oxygen saturation as the PO 2rises. Oximetry can reduce the need for arterial puncture, but arterial blood gas analysis is necessary to determine accurately the PO 2on the plateau part of the oxyhaemoglobin dissociation curve, to measure CO 2level and to assess acid/base status.
A simple algorithm for reviewing blood gas results
Most blood results in medicine are relative easy to make sense of; there’s one value, and it’s either high or low. When faced with the results of an arterial blood gas measurement, the clinician has to handle six different values, which must be drawn together and interpreted as one. The inexperienced often find their attention skipping from one number to the next, declaring each as either high or low, before becoming utterly confused and giving up. A simple stepwise system for interpreting blood results would help. The following algorithm is easy to follow and will make sense of most of the results you’ll come across in clinical practice.
1 Look at the pH. Decide whether this is an acidosis or alkalosis. Once that fact is determined, don’t be diverted from it after reviewing the other values. It won’t change. If the pH is in the normal range, note whether it is erring towards one end of the range or the other. If there is a compensated abnormality, the position of the pH within the range may indicate the nature of the primary disturbance. Remember that physiological compensatory mechanisms don’t overcompensate.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Respiratory Medicine»
Представляем Вашему вниманию похожие книги на «Respiratory Medicine» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.






Обсуждение, отзывы о книге «Respiratory Medicine» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.