Paul M. Speight - Shear's Cysts of the Oral and Maxillofacial Regions
Здесь есть возможность читать онлайн «Paul M. Speight - Shear's Cysts of the Oral and Maxillofacial Regions» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Shear's Cysts of the Oral and Maxillofacial Regions
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Shear's Cysts of the Oral and Maxillofacial Regions: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Shear's Cysts of the Oral and Maxillofacial Regions»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Shear’s Cysts of the Oral and Maxillofacial Regions
Shear’s Cysts of the Oral and Maxillofacial Regions Fifth Edition
Shear's Cysts of the Oral and Maxillofacial Regions — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Shear's Cysts of the Oral and Maxillofacial Regions», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
The inflammatory cell infiltrate in the cyst wall and the epithelial lining may vary considerably, since it reflects a single moment of the pathogenic pathway caught in a histological section. Thus any of the inflammatory cells involved in the development of the lesion may be seen. In early lesions the proliferating epithelial lining usually contains many PMNs, whereas the adjacent fibrous capsule is infiltrated mainly by chronic inflammatory cells (Shear 1963a , 1964 ; Cohen 1979 ; Matthews and Browne 1987 ). The proliferating epithelial lining shows a considerable degree of inter‐ and intraepithelial oedema or spongiosis.
The cyst wall is essentially composed of granulation tissue at various stages of maturation, depending on the age of the lesion and on the proximity to the source of the inflammation. The wall is therefore often zoned, with heavily inflamed granulation tissue adjacent to the epithelial lining, less inflamed maturing granulation tissue centrally, and collagenous fibrous tissue at the peripheral margin adjacent to the bone ( Figure 3.12). Inflammation is also more prominent adjacent to the root apex – where accumulations of polymorphs may be seen, even in long‐standing lesions. The predominant cell population, however, is of chronic inflammatory cells, mostly lymphocytes; plasma cells are also seen, and on occasion may predominate or may form dense focal accumulations.
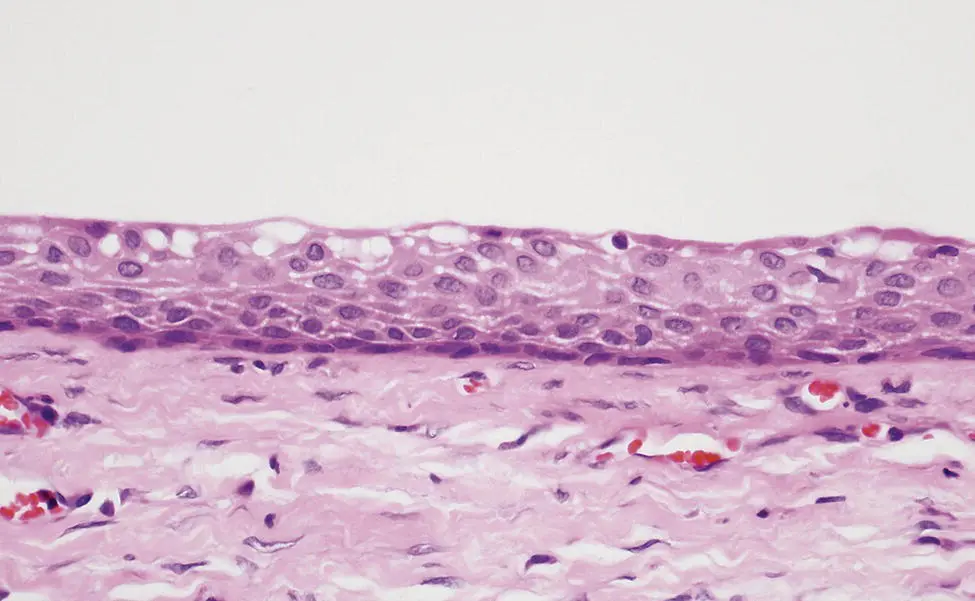
Figure 3.13 Quiescent epithelium lining a mature, long‐standing residual cyst.
Remnants of odontogenic epithelium and occasional satellite microcysts may be found in the fibrous capsule and there have been reports of examples where epithelial proliferation is so extensive that it resembles squamous odontogenic tumour (Wright 1979 ; Simon and Jensen 1985 ; Unal et al. 1987 ; Chrcanovic and Gomez 2018a ). These proliferations are reactive in nature and should not be interpreted as a co‐existent neoplasm. The behaviour is that of the cyst of origin and no further treatment is required if this observation is made during histological examination of the cyst wall (Chrcanovic and Gomez 2018a ).
Some cyst walls are markedly vascular. Haemorrhage is invariably present and haemosiderin deposits are seen in many specimens (Shear 1963c ). Calcifications of various kinds may also be seen. Dystrophic calcifications associated with necrotic and degenerative material in the cyst lumen are a particular feature of residual cysts that have been present for a long time (High and Hirschmann 1986 ). Hyaline bodies may also calcify either within the epithelial lining or among deposits that have extruded into the lumen or into the wall. In curettage specimens, trabeculae of reactive woven bone and occasionally lamellar bone are often found at the periphery of the lesion. Occasionally a well‐formed rim of woven bone may be seen.
Although well‐formed colonies of actinomycosis are well described in case reports, this is a rare finding. Hirschberg et al. (2003 ) found colonies of Actinomyces in only 17 of 936 (1.8%) periapical lesions examined, 4 of which were radicular cysts. Nair (2006 ) found a similar frequency in a review of the literature, and postulated that established colonies of Actinomyce s may persist and be an important cause of endodontic failure and persistent or recurrent lesions. Ricucci and Siqueira (2008 ), however, found no evidence for this and suggested that provided the root canal was properly cleaned, the presence of actinomycosis was not associated with treatment failure.
Cellular and Metaplastic Changes
Radicular cysts may show variable histological features due to reactive changes and to metaplastic changes of the lining epithelium. These additional features are characteristic and occasionally assist in diagnosis ( Table 3.3, Figure 3.14).
Keratin formation may occasionally be seen in radicular cysts, but when present it affects only part of the cyst wall ( Figure 3.14a). Browne and Smith (1991 ) stated that 2% of radicular cysts may show some keratinisation and that orthokeratin with evidence of a granular cell layer is most common. More recently, Maheswaran et al. (2014 ) analysed 38 radicular cysts and 9 residual cysts using Papanicolaou stain and found evidence of keratinisation in 12 (31.6%) radicular cysts and 6 (66.7%) residual cysts. Orthokeratin was only found in 1 residual cyst and only 2 cysts showed typical parakeratin. In all other cases the keratin was described as focal. However, little detail was given and the findings were not illustrated. We interpret this to mean that the Papanicolaou technique revealed occasional superficial orange‐stained cells. Although this may suggest early keratinisation, it should be noted that this technique is primarily a cytological stain and may not be as reliable as a routine haematoxylin and eosin (H&E) stain for identification of keratin in histological sections (Rao et al. 2015 ). A more cautious interpretation of Maheswaran et al.'s data may suggest that only three of their cysts showed clearly identifiable keratinisation (6.4%). Our experience would support this, since we rarely see true keratinisation in radicular cysts, and when present it affects only a small section of the lining. This, and attention to the clinical and radiological findings (association with a non‐vital tooth), should prevent the lesion being misinterpreted as odontogenic keratocyst. Also, when present the parakeratin seen in a radicular cyst is different morphologically from that seen in keratocysts, since it lacks the typical corrugated surface and affects only a small portion of the lesion.
Table 3.3 Characteristic histopathological features found in radicular cysts, with their approximate frequency (see text for explanation).
| Feature | Frequency (%) |
|---|---|
| Keratinisation | 2 |
| Ciliated cells | 10 |
| Hyaline bodies | 10 |
| Foamy histiocytes | 10 |
| Mucous cells | 20 |
| Cholesterol | 30 |
Metaplastic changes, in the form of mucous cells or ciliated cells, are frequently found in the epithelial linings of radicular cysts ( Table 3.3; Shear 1960b ; Browne 1972 ; Browne and Smith 1991 ; Slabbert et al. 1995 ; Takeda et al. 2005 ; Tsesis et al. 2016 ). Mucous cells are seen in the surface layer of the stratified squamous epithelial lining, either as a continuous row ( Figure 3.14d) or as scattered cells ( Figure 3.14c). Ciliated cells may also be seen, but are always found in association with mucous cells and together they sometimes form quite well‐developed respiratory‐type (pseudostratified columnar ciliated) epithelium ( Figure 3.14b).
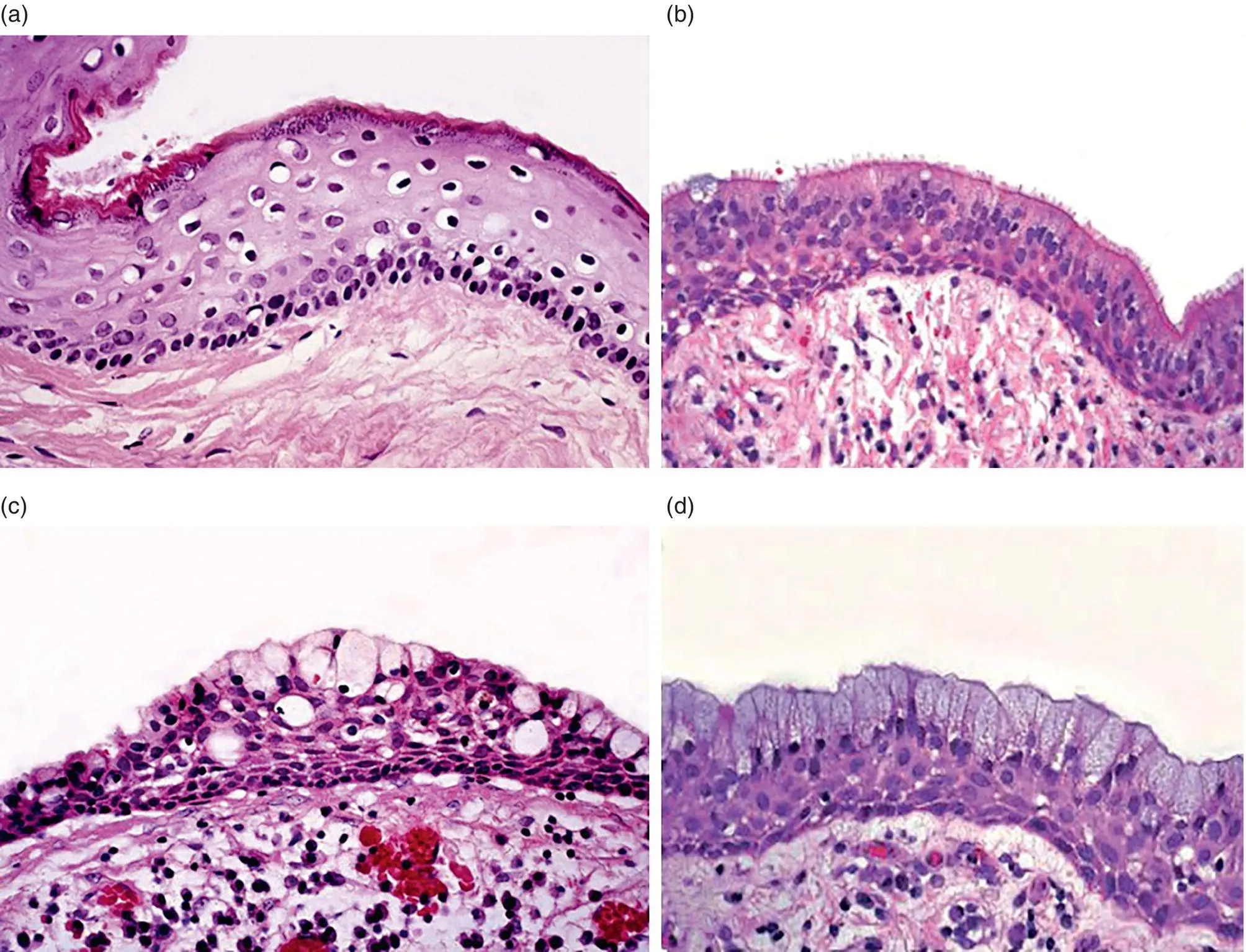
Figure 3.14 Cellular changes in the lining of radicular cysts. (a) A portion of the lining showing a focal area of orthokeratinisation. (b) Respiratory‐type epithelium with cilia and occasional mucous (goblet) cells. (c, d) Mucous cells in the surface layer may be scattered (c) or may form a continuous row (d).
Browne (1972 ) examined 402 radicular cysts and found mucous cells in 159 (39.6%), but cilia were only found in 3 cases (0.7%). Takeda et al. (2005 ) found mucous cells in 18% of radicular cysts, and in most cases they were arranged along the surface of the epithelium, but occasional intraepithelial gland‐like structures were also noted, most often in areas where the epithelium was hyperplastic. Browne (1972 ) found no difference in frequency of mucous cells between mandibular and maxillary lesions, but Takeda et al. (2005 ) found that they were more common in maxillary lesions (21%) than mandibular lesions (14%). In an analysis of 711 radicular cysts, Tsesis et al. (2016 ) found mucous cells in 5.3% and 7.4% of mandibular and maxillary lesions, respectively, but this difference was not significant. They also found that mucous cells were significantly more likely to be found in residual (23.5%) than radicular (5.8%) cysts, and were also more frequent in asymptomatic cysts and in cysts with well‐demarcated radiographic margins. This suggests that metaplasia takes time and is more likely to be encountered in well‐established or older cysts. This view is supported by the observation of Browne (1972 ) that there was an increasing frequency of mucous cells with age, at the rate of 7% per decade.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Shear's Cysts of the Oral and Maxillofacial Regions»
Представляем Вашему вниманию похожие книги на «Shear's Cysts of the Oral and Maxillofacial Regions» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.


Обсуждение, отзывы о книге «Shear's Cysts of the Oral and Maxillofacial Regions» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.