Paul M. Speight - Shear's Cysts of the Oral and Maxillofacial Regions
Здесь есть возможность читать онлайн «Paul M. Speight - Shear's Cysts of the Oral and Maxillofacial Regions» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Shear's Cysts of the Oral and Maxillofacial Regions
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Shear's Cysts of the Oral and Maxillofacial Regions: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Shear's Cysts of the Oral and Maxillofacial Regions»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Shear’s Cysts of the Oral and Maxillofacial Regions
Shear’s Cysts of the Oral and Maxillofacial Regions Fifth Edition
Shear's Cysts of the Oral and Maxillofacial Regions — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Shear's Cysts of the Oral and Maxillofacial Regions», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
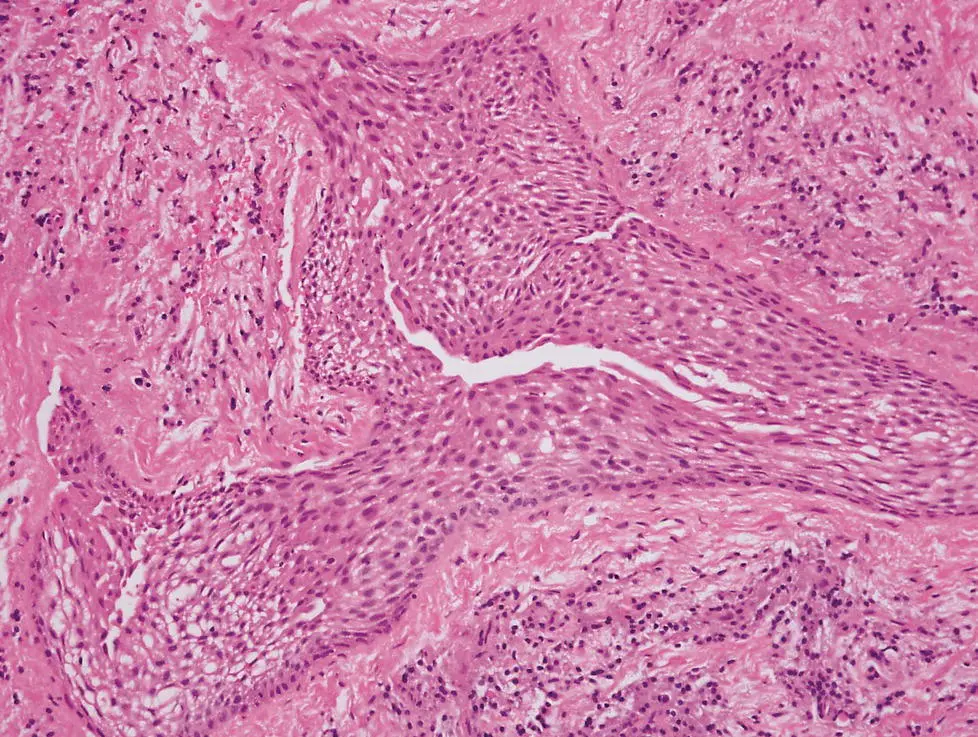
Figure 3.8 Sheet of epithelial cells in a periapical lesion. A distinct cleft has formed and this may initiate a radicular cyst.
Despite this, as described previously, there is good evidence that PMNs are a prominent feature of periapical granulomas and are associated with epithelial proliferation (Valderhaug 1972 ; Shear 1963a , 1964 ; Cohen 1979 ; Johannessen 1986 ; Marton and Kiss 2014 ). In their examination of 256 periapical lesions, Nair et al. (1996 ) showed that 90 (35%) were an ‘abscess’ and that two‐thirds of these contained epithelium. However, the definition of an abscess was of a collection of PMNs in a pre‐existing periapical granuloma – making distinction of a primary abscess from a collection of PMNs in a necrotic lesion difficult. In support of the abscess theory, Nair et al. (2008 ) were able to demonstrate that epithelium implanted into experimentally induced abscesses could form cysts. However, the relevance of these experiments is uncertain, since the abscesses were induced in the skin of experimental rats, and cysts only developed in 2 of 16 animals (6%). In addition, it is known that implanted epithelium may cause cysts even in the absence of infection or abscess formation. Nevertheless, we have seen cases of abscess formation in periapical granulomas where the abscess cavity has become encased in epithelium to form a cyst filled with PMNs ( Figure 3.10). This supports the abscess theory, but not to the exclusion of the other possible mechanisms.
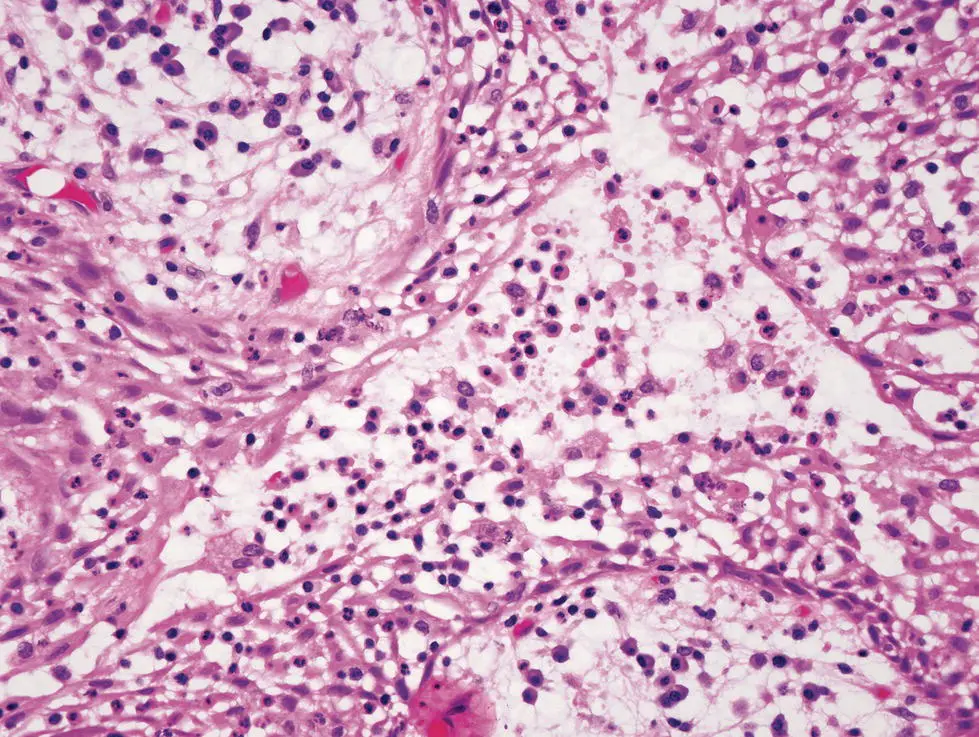
Figure 3.9 Degeneration of cells in the centre of a mass of proliferating epithelium in a periapical granuloma. There is an intense infiltration of lymphocytes and polymorphonuclear leukocytes. Accumulations of intercellular fluid coalesce to form a microcyst.
It seems, therefore, that there is little difference between the three proposed mechanisms – cyst formation occurs due to a ‘walling‐off’ of inflamed connective tissue by a process of epithelial proliferation similar to healing at an epithelial surface. This is due to the innate property of epithelium to form an external protective integument. The cyst lumen therefore represents the external environment, and in the case of a pocket or bay cyst (see later in this chapter) is continuous with the outside through the root canal. All three theories are thus tenable and not mutually exclusive. There is good observational or experimental evidence for each but, conversely, there is little evidence to refute any of them.
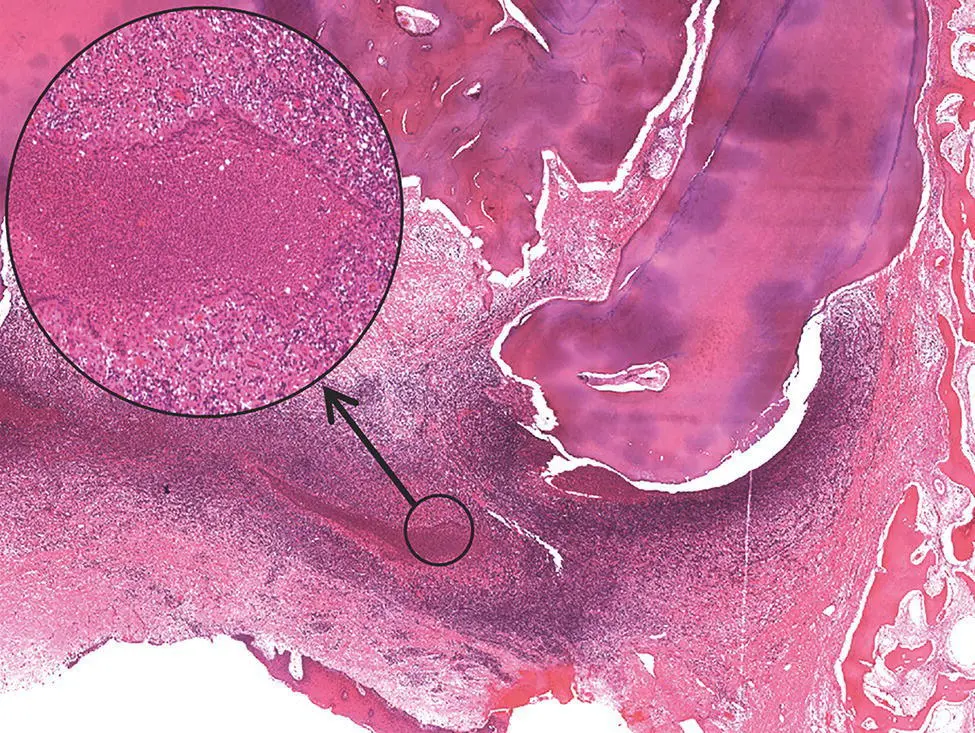
Figure 3.10 A periapical granuloma at the apex of a molar tooth root. There is a central focal accumulation of polymorphonuclear leukocytes that has become surrounded by epithelium (inset).
Growth and Enlargement of the Radicular Cyst
Role of Hydrostatic Pressure
The third phase in the pathogenesis of the radicular cyst is its growth and enlargement, which must involve a mechanism for expansion and for resorption of alveolar bone. Almost without exception, radicular cysts, especially when small, are seen as round or spherical radiolucencies on radiographs and on 3D imaging (CT or CBCT). This implies that growth of the cyst is regular and centripetal, and it is widely accepted that hydrostatic pressure, due to osmosis, provides the slow and evenly distributed forces necessary to achieve this growth pattern. This was first noted by Warwick James in 1926 in an address to the Royal Society of Medicine. He also reported that he had measured the increased pressure in cysts and was probably the first to suggest that ‘The increase in tension may be partly due to osmosis’ (Warwick James 1926 ). (Many of these very early papers are freely available online and are recommend for their clarity, insight, and the quality of the scientific observations.) The evidence for this was provided by early experiments carried out by Paul Toller, more than half a century ago, which have never been repeated or bettered (Toller 1948 , 1966b , 1967 , 1970a , 1970b ). In his first paper, Toller noted that early surgeons had observed that when opened, jaw cysts appeared to be under pressure, and that marsupialisation checked further growth and led to a reduction in size of the lesions (Toller 1948 ). He quoted Potts, who in 1927 had noted that cysts displaced the roots of teeth ‘as if by pressure’. This led to his experiments to measure the hydrostatic pressure in jaw cysts. Using a cannula and a manometer, he showed that the intracystic pressure in radicular and dentigerous cysts averaged 65–70 cm of water, which was considerably higher than capillary blood pressure, which was estimated to be lower than 10 cm of water (Toller 1948 ). In the same paper, he suggested that this increased pressure was a result of ‘osmotic tension’ and then went on to test whether the cyst lining acted as a semi‐permeable membrane. He used freshly dissected walls from radicular cysts and clamped them between two cylinders of Ringer's solution with 5% albumin added to one side. In all cases fluid passed through the cyst wall towards the albumin, showing that the wall acted as a semi‐permeable membrane.
In later studies, Toller (1970b ) showed that the mean osmolality of the fluid from 21 apical and residual cysts was 290 ± 14.93 mOsm and was greater than the mean serum osmolality of 279 ± 4.68 mOsm ( P < 0.01). Lytic products of the epithelial and inflammatory cells in the cyst cavity provided the great numbers of smaller molecules that raised the osmotic pressure of the cyst fluid. Toller believed that the upper limit of permeability in most cysts was close to the molecular size of albumin (molecular weight 69 kDa) and that particles of larger size would find difficulty in diffusing across a cyst lining. These findings were confirmed by Skaug (1976a ), who conducted similar experiments and showed that the intracystic pressure ranged from 25 to 66 mmHg and that these pressures were restored 3–7 days after aspiration, suggesting that there was constant movement of fluid into the cyst lumen.
This pioneering work on the role of hydrostatic pressure in the growth of odontogenic cysts was mostly undertaken during the 1970s, but it has not been superseded or refuted by more contemporary experiments. Nair (1998 , 2004 ) has suggested that osmotic pressure as a factor in the development of radicular cysts has been ‘eliminated’. As evidence for this he cites the fact that the lumen of pocket or bay cysts is open to the root canal, and cannot therefore sustain an increased internal pressure. He suggests that cyst growth is sustained by molecular mechanisms. This is undoubtedly correct – a cascade of biological factors underpins the processes of epithelial proliferation, extracellular matrix destruction, and bone resorption, but there is still good evidence that there is increased pressure within the cyst lumen, and that osmosis is the driving force. This does not exclude other factors, although it should be noted that even in pocket cysts it is unlikely that the root canal remains empty and that the lumen is truly open to the oral cavity. It is also well recognised that release of this pressure, through decompression, has long been and still is a common and effective form of treatment (Castro‐Núñez 2016 ). More recently this issue has been re‐evaluated, but the outcome remains that hydrostatic pressure is still considered to be of primary importance in the growth of all cyst types. Kubota et al. (2004 ) measured the intracystic fluid pressure of odontogenic keratocysts, dentigerous cysts, and radicular cysts. They confirmed the earlier results of Toller (1970b ) and Skaug (1976a ), that the pressure was greater than the local blood pressure and that there were no differences between the three cyst types. They also measured cyst volume and showed that volume correlated to the area of the cysts measured on panoramic radiographs. They correlated the pressure to the areas of the cysts and found pressures of 337.6 ± 126.0, 258.2 ± 160.9, and 254 ± 157.3 mmHgcm −2for keratocysts, dentigerous cysts, and radicular cysts, respectively. Furthermore, these authors showed that the intracystic pressure in all cyst types was inversely correlated to the cyst size. They therefore concluded that increased pressure played a pivotal part in early cyst growth.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Shear's Cysts of the Oral and Maxillofacial Regions»
Представляем Вашему вниманию похожие книги на «Shear's Cysts of the Oral and Maxillofacial Regions» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.


Обсуждение, отзывы о книге «Shear's Cysts of the Oral and Maxillofacial Regions» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.