Managing Medical and Obstetric Emergencies and Trauma
Здесь есть возможность читать онлайн «Managing Medical and Obstetric Emergencies and Trauma» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Managing Medical and Obstetric Emergencies and Trauma
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Managing Medical and Obstetric Emergencies and Trauma: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Managing Medical and Obstetric Emergencies and Trauma»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
MANAGING MEDICAL AND OBSTETRIC EMERGENCIES AND TRAUMA A PRACTICAL APPROACH
provides an evidence-based, structured approach to the recognition and treatment of emergencies in pregnancy. This contemporary resource provides step-by-step guidance on the knowledge, practical skills and procedures required to improve outcomes for the mother and fetus. Now in its fourth edition, the text fully aligns with the mMOET course, and has been extensively reviewed and revised throughout. Lessons learned from mortality reports and national guidelines underpin the new material. This edition includes: New chapters on cardiac disease, neurological emergencies and human factors An update for obstetric teams treating pregnant trauma patients in line with modern trauma management Revised algorithms and new illustrations
is a vital source of practical information presented as a systematic approach to prepare the obstetric team: obstetricians, midwives, anaesthetists and emergency physicians. The Advanced Life Support Group (ALSG)
Managing Medical and Obstetric Emergencies and Trauma — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Managing Medical and Obstetric Emergencies and Trauma», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
7.4 Microbiology
A study of severe maternal sepsis in the UK (2011–2012) identified genital tract infection (31%) and the organisim Escherichia coli (21%) to be the most common causes, followed by group A Streptococcus , group B Streptococcus , other streptococci and Staphylococcus . Risk factors for severe sepsis were if the woman was black or of other ethnic minority, primiparous, had a pre‐existing medical problem, had a febrile illness or were taking antibiotics in the 2 weeks preceding presentation, operative vaginal delivery or caesarean. Median time between delivery and sepsis was 3 days. Multiple pregnancy and group A Streptococcus were associated with progression to septic shock. In the women with group A streptococcal infection the progression of sepsis was often rapid . For each maternal sepsis death, 50 women had life‐threatening morbidity from sepsis.
A study from Ireland (2005–2012) looking at maternal bacteraemia again found E. coli to be the predominant pathogen followed by group B Streptococcus . The source of infection was the genital tract in 61% of cases and the urinary tract in 25%; 17% of sepsis episodes occurred antenatally, 36% intrapartum and 47% postpartum. Sepsis was associated with preterm delivery and a high perinatal mortality rate. The most virulent organisms were group A streptococci associated with postpartum sepsis at term and E. coli sepsis preterm.
Group A Streptococcus is a common skin or throat commensal, carried asymptomatically by up to 30% of the population. It is easily spread and is responsible for streptococcal sore throat, a very common childhood condition. Worldwide, however, group A Streptococcus is still the most common cause of postpartum maternal death and can kill pregnant and recently pregnant women with devastating speed. The initial presentation can be vague and non‐specific, thus delaying treatment. Primary symptoms include myalgia, fever, mild confusion, dizziness and abdominal pain.
Transmission in pregnant women is thought to be either through the blood stream with the throat as a portal of entry, or via the perineal route with translocation from colonisation in the vagina, even in the presence of an intact membrane, as bacteria can cross this apparent barrier. Translocation from the vagina may occur from nosocomial exposure at birth or via a caesarean section incision. Streptococcal infection has a seasonal rise in incidence between December and April in the northern hemisphere. The link between pregnant women and children with group A streptococcal sore throats is thought to be significant as a possible source of infection.
In the past, there was an emphasis on the transmission of infection from care‐givers to women, much reduced since the advent of strict hygiene practices in hospitals. It is thought that raising public health awareness of the risks from family members and encouraging women to follow appropriate personal hygiene practices may be helpful in reducing transmission of infection; in particular, pregnant women should be encouraged to handwash both before and after using the toiletto avoid transmitting organisms from other household members.
7.5 Clinical issues and presentation
Minimising risk from infection in the antenatal period, by avoiding unnecessary vaginal examinations and paying attention to hygiene, may reduce the incidence of sepsis. Early recognition and increased surveillance of those at risk including careful assessment of postnatal mothers, especially those with prolonged rupture of membranes, ragged membranes or possible incomplete delivery of the placenta and women with uterine tenderness or enlargement, will help to identify women developing serious infection. Multiple presentations should be seen as a red flag and requires careful review with escalation to senior staff for assessment.
Symptoms of sepsis may include:
Feeling unwell, anxious or distressed
Shivery or feverish
Sore throat, cough or influenza‐like symptoms (pneumonia accounts for a significant number of admissions to the intensive care unit in pregnant women in the antenatal period)
Rash (see Appendix 7.1for weblink to assessment of pregnant woman reporting viral rash illness)
Chest pain
Vomiting and/or diarrhoea
Abdominal pain, uterine and renal angle pain, and beware ‘after pains’ of a severity that is out of proportion to the known cause and not responding to usual analgesia
Wound tenderness
If pregnant may report reduced fetal movements
Offensive vaginal discharge
Persistent vaginal bleeding may be a sign of uterine sepsis
Breast tenderness, suggesting mastitis
Headache
Unexplained physical symptoms
A high index of suspicion and close surveillance will help in identifying women with early sepsis. When assessing a woman who is unwell, revisit the history and consider her clinical condition in addition to the modified early obstetric warning score (MEOWS) and do not be reassured by a single set of observations on the MEOWS chart (Knight et al., 2017). Chronic illness and immunosuppression are risk factors for sepsis. Immunosuppression puts a woman at higher risk of rapid deterioration from sepsis, and sepsis should be considered a likely cause when they are unwell.
Serious clinical signs can be categorised as red and amber flags.
The Sepsis Trust UK Sepsis Screening Tool for Acute Assessment of the pregnant or up to 6 weeks’ post‐pregnancy woman is reproduced in Figure 7.2and defines the red and amber flags.
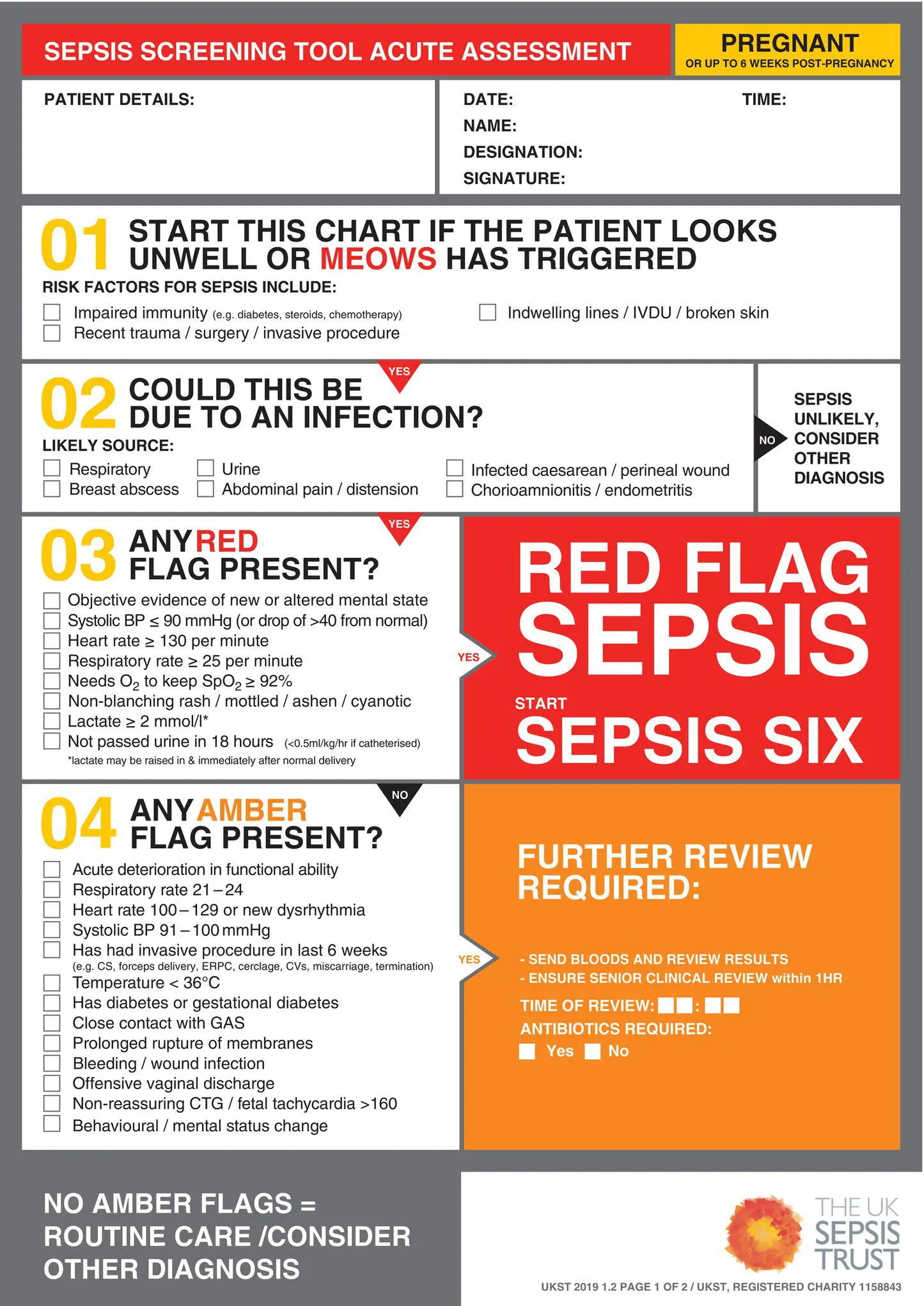
Figure 7.2 Sepsis Trust UK Sepsis Screening Tool for Acute Assessment
Source : Nutbeam T, Daniels R on behalf of the UK Sepsis Trust. © 2019 UK Sepsis Trust
7.6 Monitoring, investigations and urgent treatment
Monitor women who have red and amber flags with suspected sepsis continuously and record using a MEWS chart (NICE, 2016). The conscious level should also be monitored using ACVPU( alert, new confusion, responds to voice, responds to pain, unconscious). A sepsis care bundlemust be applied in a structured and systemic way with urgency.The time to administration of antibiotics is a predictor of mortality in sepsis, do not delayand use local antibiotic prescribing guidance. Antiviral medication may also be appropriate. The woman must be continually reassessed and senior reviewis essential. Consider ‘declaring sepsis’, analogous to activation of the major obstetric haemorrhage protocol.
The UK Sepsis Trust recommends the Sepsis Six ( Algorithm 7.1) with all actions to be completed within 1 hour.
You can think of it as:
‘3 in, 3 out”: fluids, antibiotics and oxygen in / catheter, lactate and blood cultures out.
Initial blood tests include lactate– either arterial if there is evidence of hypoxia or a venous sample. Any woman in whom sepsis is suspected, who has a lactate >2 mmol/l, needs to have resuscitation started immediately. Raised serum lactate is a marker for poor perfusion and tissue hypoxia from whatever cause and signifies severe illness.
Additional blood tests include blood cultures, full blood count, coagulation screen, urea and electrolytes, blood glucose, liver profile and C‐reactive protein (CRP). Consider urinalysis, urine for culture, sputum culture, vaginal swabs, breast milk culture and throat swabs. Consider a chest x‐ray in all with suspected sepsis. Consider imaging of the abdomen and pelvis if no likely source of infection is identified after clinical examination and initial tests.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Managing Medical and Obstetric Emergencies and Trauma»
Представляем Вашему вниманию похожие книги на «Managing Medical and Obstetric Emergencies and Trauma» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.






Обсуждение, отзывы о книге «Managing Medical and Obstetric Emergencies and Trauma» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.