Managing Medical and Obstetric Emergencies and Trauma
Здесь есть возможность читать онлайн «Managing Medical and Obstetric Emergencies and Trauma» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Managing Medical and Obstetric Emergencies and Trauma
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Managing Medical and Obstetric Emergencies and Trauma: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Managing Medical and Obstetric Emergencies and Trauma»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
MANAGING MEDICAL AND OBSTETRIC EMERGENCIES AND TRAUMA A PRACTICAL APPROACH
provides an evidence-based, structured approach to the recognition and treatment of emergencies in pregnancy. This contemporary resource provides step-by-step guidance on the knowledge, practical skills and procedures required to improve outcomes for the mother and fetus. Now in its fourth edition, the text fully aligns with the mMOET course, and has been extensively reviewed and revised throughout. Lessons learned from mortality reports and national guidelines underpin the new material. This edition includes: New chapters on cardiac disease, neurological emergencies and human factors An update for obstetric teams treating pregnant trauma patients in line with modern trauma management Revised algorithms and new illustrations
is a vital source of practical information presented as a systematic approach to prepare the obstetric team: obstetricians, midwives, anaesthetists and emergency physicians. The Advanced Life Support Group (ALSG)
Managing Medical and Obstetric Emergencies and Trauma — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Managing Medical and Obstetric Emergencies and Trauma», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
In 2017 the World Health Organization (WHO) defined maternal sepsis as a life‐threatening condition defined as organ dysfunction resulting from infection during pregnancy, childbirth, post‐abortion, or postpartum period( Figure 7.1).
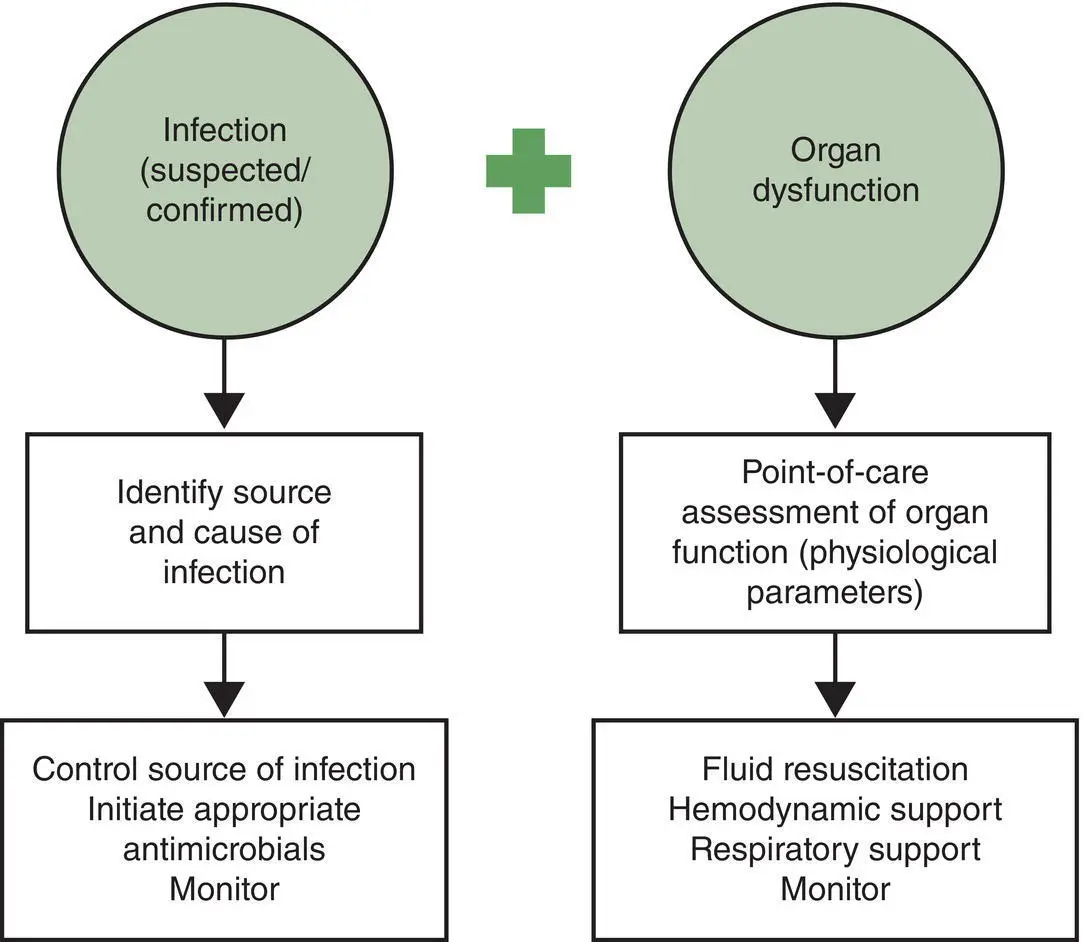
Figure 7.1 Approach for implementation of the new WHO definition of maternal sepsis
Source : Statement on maternal sepsis, WHO. © 2017 WHO
The Third International Consensus (2016) definition of sepsis (SEPSIS‐3) for the whole adult population is that sepsis is a life‐threatening organ dysfunction due to a dysregulated host response to infection.
Septic shockis a life‐threatening condition that is characterised by low blood pressure despite adequate fluid replacement, and organ dysfunction or failure. The Third International Consensus definition (SEPSIS‐3) of septic shock is persisting hypotension requiring vasopressors to maintain mean arterial pressure of 65 mmHg or more and having a serum lactate of greater than 2 mmol/l despite adequate volume resuscitation.
These definitions depend on the identification of organ dysfunction in the presence of infection. In the general adult population, a brief bedside tool such as the quick SOFA ( sequential organ failure assessment) or qSOFA score is used as described in SEPSIS‐3. The qSOFA score evaluates the presence of three clinical criteria: systolic blood pressure ≤100 mmHg, respiratory rate ≥22 per minute and altered mental status. If two or more of these criteria are present the patient is at increased risk of a poor sepsis‐related outcome and urgent action is prompted. An obstetric modified qSOFA has been produced by the Society of Obstetric Medicine Australia and New Zealand and modifies the systolic blood pressure to ≤90 mmHg, respiratory rate ≥25 per minute and altered mental state. Table 7.1summarises the organ damage by system caused by sepsis.
Table 7.1 Organ damage caused by sepsis
Source : Plant LA, Pacheco LD, Louis JM. Sepsis during pregnancy and the puerperium. SMFM Consult Series No. 47: Am J Obstet Gynecol 2019; 220(4): B2–B10. © 2019 Elsevier
| Organ system | Clinical features |
|---|---|
| Central nervous system | Altered mental status |
| Cardiovascular system dysfunction | Hypotension from vasodilatation and third spacing; myocardial |
| Pulmonary system | Acute respiratory distress syndrome (ARDS) |
| Gastrointestinal | Paralytic Ileus |
| Hepatic system | Hepatic failure or abnormal transaminases |
| Urinary system | Oliguria or acute kidney injury |
| Haematological system | Thrombocytopenia or disseminated intravascular coagulation |
| Endocrine system | Adrenal dysfunction and increased insulin resistance |
Although people with sepsis may have an infection, fever is not always present . The signs and symptoms of sepsis can be non‐specific and can be missed if clinicians do not think ‘Could this be sepsis?’
The key actions for the diagnosis and management of sepsis(Knight et al., 2014, 2017) are:
Timely recognition
Fast administration of antibiotics
Quick involvement of experts – senior review is essential
7.2 Sepsis in pregnancy
Pregnant women have increased susceptibility to some infectious diseases, e.g. Plasmodium falciparum and Listeria monoctogenes
In advanced pregnancy there are immunological changes that decrease adaptive immunity such that increased severity of infection is seen where cell‐mediated immunity is important. Pregnant women are more severely affected by influenza virus, hepatitis E virus, herpes simplex virus and malaria parasites
The physiological changes of pregnancy that reduce lung capacity and promote urinary stasis may promote more severe infection
The 2014 MBRRACE‐UK report highlighted a substantial number of women who died following infection with influenza and the recommendation was made for influenza vaccination in pregnancy. The 2017 MBRRACE‐UK report re‐emphasised that pregnant women with influenza were dying from a vaccine preventable diseaseand that the messages around vaccination and treatment of influenza needed to be embedded to prevent deaths and to prepare for a future pandemic. Staff should remain aware of the possibility of influenza infectionespecially during peak seasonal periods. The Covid‐19 pandemic has highlighted these messages once again.
Antepartum causes of sepsis are commonly non‐pelvic in origin. Intrapartum and postpartum sepsis is more likely to be pelvic in origin. The classification of maternal infection is given in Box 7.1.
Box 7.1Classification of maternal infection aligned with the WHO classification of maternal death
1 Pregnancy‐specific infections:ChorioamnionitisEndometritisLactational mastitisSite of perineal traumaSurgical site, e.g. caesarean
2 Infections exacerbated by pregnancy, including:Urinary tract infectionInfluenzaListeriosisHepatitis EHerpes simplex virusMalaria
3 Incidental infections, including:Lower respiratory tract infectionsAcute appendicitisAcute cholecystitisAcute pancreatitisNecrotising fasciitisTuberculosisSexually transmitted diseases
Source : Turner MJ. Maternal sepsis is an evolving challenge. Int J Gynecol Obstet 2019: 146: 39–42. © 2019 John Wiley & Sons
7.3 Pathophysiology of sepsis
Once an infective agent enters the body it binds to the surface of immune cells such as macrophages and monocytes and initiates the immune and coagulation cascades. This involves the release of both pro‐ and anti‐inflammatory cytokines along with pro‐coagulant mediators which activate the extrinsic coagulation pathway and inhibit fibrinolysis. Infection becomes sepsis when the balance of pro‐ and anti‐inflammatory mechanisms tips towards pro‐inflammation.
The pro‐inflammatory cytokines cause endothelial dysfunction and leaky capillaries resulting in vasodilatation and maldistribution of fluid. Activation of the extrinsic coagulation cascade and inhibition of fibrinolysis results in the formation of thrombi in the microcirculation. These thrombi then compromise organ perfusion, resulting in impaired delivery of oxygen to tissues and organs. If unchecked, this can lead to multiorgan failure and ultimately death.
Clinical manifestations of haemodynamic alterations
There is a decrease in arteriolar and venous tone. This causes venous pooling of blood and a drop in vascular resistance, resulting in hypotension. In the initial stages of sepsis, there is hypotension with reduced cardiac output and low filling pressures. With fluid resuscitation, cardiac output increases, resulting in a hyperdynamic circulation, but there is not much change in blood pressure owing to a reduced vascular resistance. There is an increase in pulmonary vascular resistance, resulting in raised pulmonary arterial pressures. The changes in the vascular tone differ in different vascular beds, resulting in the maldistribution of blood volume and flow. There is evidence to suggest that the ability of tissues to extract oxygen is impaired owing to mitochondrial dysfunction. This encourages anaerobic metabolism in tissues, promoting lactic acidosis.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Managing Medical and Obstetric Emergencies and Trauma»
Представляем Вашему вниманию похожие книги на «Managing Medical and Obstetric Emergencies and Trauma» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.






Обсуждение, отзывы о книге «Managing Medical and Obstetric Emergencies and Trauma» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.