David Linden - Touch
Здесь есть возможность читать онлайн «David Linden - Touch» весь текст электронной книги совершенно бесплатно (целиком полную версию без сокращений). В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Год выпуска: 2014, ISBN: 2014, Издательство: Penguin Books Ltd, Жанр: Психология, Биология, sci_popular, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Touch
- Автор:
- Издательство:Penguin Books Ltd
- Жанр:
- Год:2014
- ISBN:9780241184059
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Touch: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Touch»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Dual-function receptors in our skin make mint feel cool and chili peppers hot. Without the brain’s dedicated centers for emotional touch, an orgasm would feel more like a sneeze—convulsive, but not especially nice. From skin to nerves to brain, the organization of our body’s touch circuits is a complex and often counterintuitive system that affects everything from our social interactions to our general health and development.
In Touch, neuroscientist and bestselling author David J. Linden explores this critical interface between our bodies and the outside world, between ourselves and others. Along the way, he answers such questions as: Why do women have more refined detection with their fingertips than men? Is there a biological basis for the use of acupuncture to relieve pain? How do drugs like Ecstasy heighten and motivate sensual touch? Why can’t we tickle ourselves? Linking biology and behavioral science, Touch offers an entertaining and enlightening answer to how we feel in every sense of the word.
Touch — читать онлайн бесплатно полную книгу (весь текст) целиком
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Touch», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Can orgasms occur even with no involvement of the genitals? Absolutely. 23Some people can achieve orgasm from touching areas of skin that are far from the pelvis, like the nipple, neck, mouth, and even such ostensibly nonerotic areas as the nose and the knee. 24And of course, both men and women can have orgasms from stimulation of the anus and rectum, but this is likely due to cross talk between the genital and perigenital regions, as we’ve discussed (figure 4.3). In rare cases, even touching of any kind may be dispensable. Some people appear to be able to have orgasms through thought alone, or through ritualized breathing. And, of course, orgasms can occur during sleep, even when the genital area is not in contact with bedclothes. People with complete spinal cord injuries, who cannot feel their pelvic regions at all, report orgasms during dreaming sleep that feel as if they were occurring in the genitals. 25

A group of men and women were asked to write paragraph-length descriptions of their own orgasms. Then the paragraphs were edited to remove any words (like penis or vagina) that would give a clue to the writer’s sex. When the redacted paragraphs were given to a panel of judges (composed of medical students, psychologists, and gynecologists) to analyze, the descriptions of male and female orgasms were indistinguishable. 26There are some important differences between them, however. On average, women’s orgasms, as measured using a sensor that detects involuntary contractions of rectal muscles, are somewhat longer than men’s (about twenty-five seconds, compared with fifteen seconds). Women are also much more likely to achieve orgasm more than once during a sexual encounter.
Sigmund Freud pronounced that while a young woman might achieve orgasm through clitoral stimulation, a mature woman had orgasms only when her vagina, but not her clitoris, was stimulated. He did not base this notion on anatomical or physiological measurements of the vagina or clitoris or the nerves that innervate them. Rather, he was motivated to construct a narrative in which penetration by a man’s penis was crucial for a woman’s sexual satisfaction. For their part, however, women are well aware that for most of them, young or mature, stimulation of the external clitoris, either during solo or partnered sex, is the most reliable path to achieving orgasm. This is not surprising: As we have discussed, the high density of free nerve endings and genital end bulbs in the external clitoris is consistent with its special role in sexual sensation.
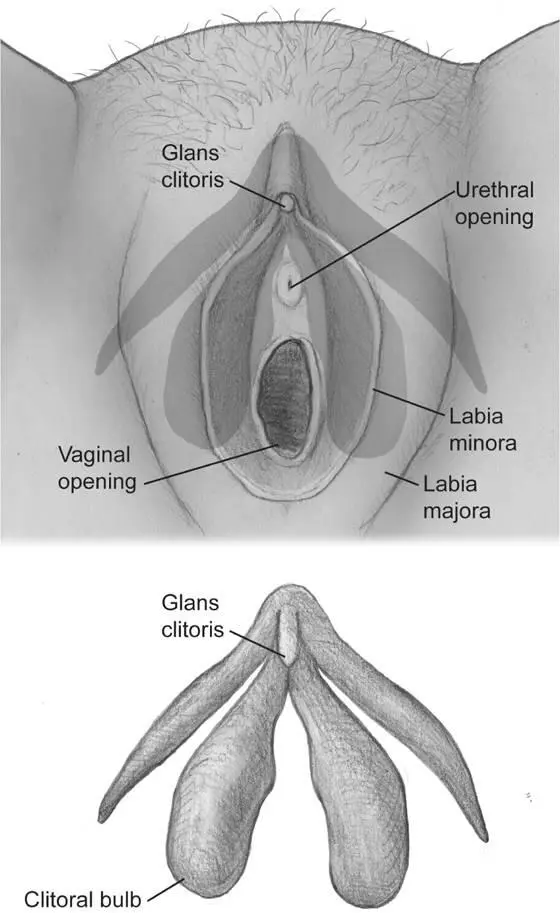
Figure 4.6The anatomy of the clitoris in relation to the urethra and vagina. Top: The external portion of the clitoris (the clitoral glans) is a small part of the entire structure shown with shading. Importantly, the base of the clitoris contacts the anterior wall of the vagina. Bottom: Here, the entire clitoris is shown with other structures removed to clearly reveal its shape. In a chronic inflammatory skin disorder called lichen sclerosus, the clitoral hood can sometimes fuse with the surrounding labia minora to completely cover the external clitoris (similar fusion of the labia can partially or completely obstruct the vaginal opening). Even when the external clitoris is overgrown with skin, most women with lichen sclerosus are still able to achieve orgasm through indirect clitoral stimulation. 27© 2013 Joan M. K. Tycko
Many years later the reaction against Freud’s “vaginal orgasm” was vociferous, reaching its peak with the publication of “The Myth of the Vaginal Orgasm” by feminist scholar Anne Koedt in 1970. 28Here the pendulum of thought swung far in the other direction. Koedt and others claimed that the clitoris was the only structure capable of transmitting women’s sexual sensation and thereby triggering orgasm. Koedt cited pioneering sex researcher Alfred Kinsey, who stated that “[the vagina is] like all other internal body structures, poorly supplied with the end organs of touch.” 29This is simply not true. While the innervation of the vaginal walls and the cervix is much less dense than that of the external clitoris, significant sensory information is conveyed from those regions. Selective stimulation of the vaginal walls and the cervix (as well as the labia, perineum, anus, and rectum) can produce clearly detectable sensations as well as localized activation in the somatosensory cortex of the brain (figure 4.4). Furthermore, we now have a better understanding of the anatomy of the clitoris. The external clitoris, a portion of the clitoral glans, is merely the “tip of the iceberg.” The deeper portions of the clitoris have a wishbone shape, comprising two bulbs that encompass the urethra and the anterior wall of the vagina (figure 4.6). As a result, stimulation of the anterior vaginal wall (the belly side) can activate sensory nerve endings in the bulbs of the clitoris. 30
Perhaps the strongest evidence for a purely vaginal orgasm that does not involve the clitoris comes from women with complete spinal cord transection. For these women, touch signals from the clitoris (both the external and the deep portions), carried by the pudendal nerve, cannot reach the brain and therefore cannot be perceived. Some of them can achieve orgasm (verified by brain scanning) from stimulation of the cervix, 8presumably due to the spared vagus nerve pathway to the brain (figure 4.3). This finding argues strongly for the existence of sexual sensation from the cervix, but does not answer the question of the role of this sensation in the orgasms of uninjured women.
While the existence of the vaginal orgasm as a unique nonclitoral physiological phenomenon continues to be a source of debate, 31several points are now clear. The clitoris has a special role in triggering orgasm via the pudendal nerve, and it may be achieved most reliably through stimulation of the external clitoris, where the density of sensory innervation is the highest. Penetration of the vagina, as occurs during dildo play, manual stimulation, or penis-vagina sex, can activate touch sensors in the base of the clitoris through the vaginal wall. It can also activate touch sensors in the vaginal wall itself, as well as those in the cervix, and these signals are conveyed to the spinal cord through different sensory nerves: the pelvic, hypogastric, and vagus. Those nerves also carry signals from perigenital areas like the perineum, rectum, and anus. Touch signals from all of these sources can contribute to orgasm.
Individual women report a great deal of variation in their experience of orgasm. For some, all orgasms feel more or less the same, while others report qualitatively different types of orgasmic sensations (focused versus spreading, convulsive versus vibrating), depending upon the details of sexual stimulation (with and without penetration, or with and without concomitant breast stimulation, for example). And, of course, cognitive and experiential factors also play an important role. I knew a woman in college who claimed that she could have an orgasm with a man only if he was wearing a singlet made of fishnet fabric. It’s unlikely that the basis for this particular erotic requirement lay in the structure of the nerve endings in her skin. A brief perusal of the Internet will yield a nearly infinite variation of requirements for orgasm in both men and women involving fantasy, role play, costumes, etc., most of them unrelated to touch sensation at all.
Generally speaking, men report more reliable orgasms than women during both masturbation and partnered sex. This has led to the popular idea that, while women experience a complex blend of sexual sensations from different pelvic areas, the entirety of men’s sexual sensation is unvarying and originates from the penis. This is incorrect. Just as the external clitoris has a special role in women’s orgasm, the penis, particularly the glabrous skin of the glans penis, is the most reliable trigger of men’s orgasm, but other pelvic regions also contribute. After complete removal of the prostate, in the best cases erection, urinary control, and orgasm are spared but ejaculation is eliminated, resulting in dry orgasms. 32In one recent small survey, all the men who had undergone complete prostatectomy but could still have orgasms reported that they no longer felt the exquisite sensation of inevitability, the “point of no return” leading to orgasm. 33Signals from the scrotum, testicles, perineum, anus, and rectum can also contribute to male orgasm and can influence both its timing and qualitative aspects (deep versus surface, throbbing versus flowing). 34
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Touch»
Представляем Вашему вниманию похожие книги на «Touch» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.





Обсуждение, отзывы о книге «Touch» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.