Point-of-Care Ultrasound Techniques for the Small Animal Practitioner
Здесь есть возможность читать онлайн «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Point-of-Care Ultrasound Techniques for the Small Animal Practitioner
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Point-of-Care Ultrasound Techniques for the Small Animal Practitioner: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
New chapters in
cover ultrasound-guided nerve blocks, musculoskeletal, brain imaging, and applications of focused ultrasound techniques in cats, exotics and marine mammals—making it an essential purchase for veterinarians wanting to incorporate point-of-care ultrasound techniques into their veterinary practices.
Presents a standardized approach to point-of-care ultrasound as an extension of the physical exam, including trauma, non-trauma, and monitoring applications Includes coverage of new techniques for focused ultrasound exams, including lung, anesthesia and ultrasound guided nerve blocks, transcranial brain imaging, musculoskeletal, volume status evaluation, and rapid assessment for treatable forms of shock Adds cats, exotic and wildlife mammals, and marine mammals to the existing canine coverage Emphasizes the integration of point-of-care ultrasound techniques for optimizing patient care and accurate patient assessment Offers access to a companion website with supplementary video clips showing many clinically relevant didactic examples The second edition of
is an excellent resource for veterinary practitioners, ranging from the general practitioner to nearly all clinical specialists, including internal medicine, oncology, cardiology, emergency and critical care, anesthesiology, ophthalmology, exotics, and zoo medicine specialists, and veterinary students.
Point-of-Care Ultrasound Techniques for the Small Animal Practitioner — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
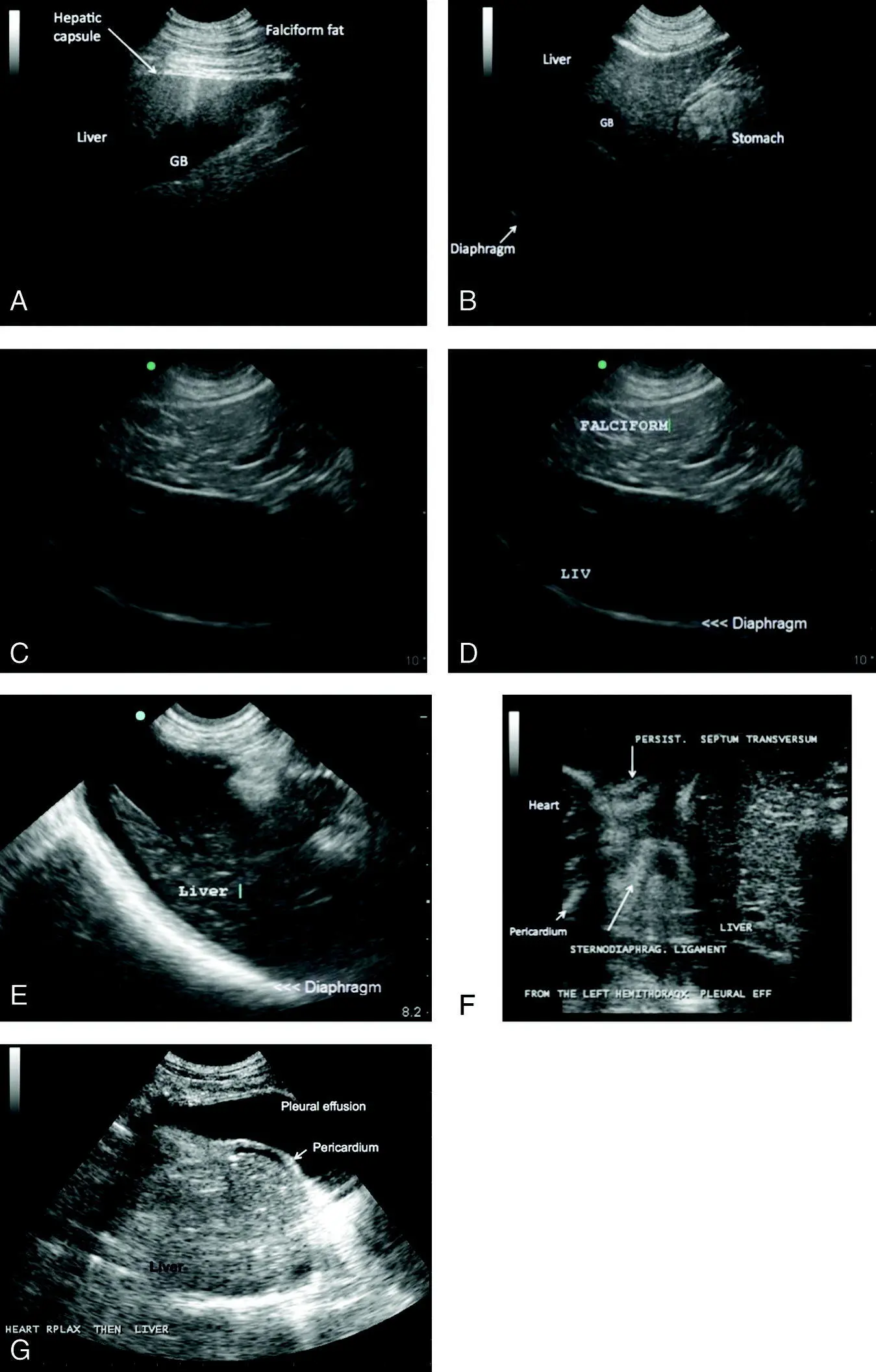
Figure 8.2. Liver margination and comparative echogenicity to the falciform fat. (A) Image of the falciform fat. Note the linear subcutaneous facial planes and falciform fat just distal to the point of probe contact. Liver echogenicity can be similar to the falciform fat. This especially depends on sonographic gain settings and hence comparative echogenicity can vary. Notice delineation between the falciform fat and normal liver by the thin echogenic line ( arrow ) representing the liver capsule. (B) Another example of differences in echogenicity between the liver and falciform fat. Note the sharp, normal liver margin. Compare to (A) and (B) and note that the liver capsule can be seen surrounding the hepatic parenchymal and at its contact with the diaphragm as a hyperechoic line (<<<). (C) Example of prominent falciform fat in a more obese patient. The falciform in the near‐field is juxtaposed to normal liver in the far field. (D) Same image as in (C) but labeled. (E) Delineation of the liver lobes is not sonographically readily apparent unless anechoic free fluid (*) (ascites) is present, as is the case in this image of a peritoneal pericardial hernia in a cat. Normally the caudal margins of the liver lobes are easily identified and sharply demarcated. Imaging of the liver should be deep enough to appreciate the diaphragm. The sharply marginated hyperechoic curvilinear structure is the liver and diaphragm interface (<<<). (F) Although not the gold standard for evaluation of diaphragmatic integrity, evaluation of the diaphragm can be useful in trauma cases and cases in which the integrity of the diaphragm may be compromised (e.g., congenital or acquired types of diaphragmatic hernia). Shown here is a peritoneal pericardial hernia in a cat. Note the embryological persistence of the septum transversum. In this patient, the liver would dynamically slip into the pericardial sac, depending on how the patient was positioned. In many cases, other abdominal organs (such as the spleen, liver or bowel) can be seen within the pericardial sac. These can be an incidental finding or seen in patients with exercise intolerance or respiratory distress. (G) Another example of a peritoneal pericardial diaphragmatic hernia in a cat with concurrent pleural effusion. The apex of the heart is identified to the left of the image. However, the homogeneously echotextured, more solid liver partially occupies a large portion of the pericardial sac. The small bowel is also commonly herniated and easily recognized by the layering of its walls.
Ultrasonographic Findings: Normal Liver and Gallbladder
The liver is composed of six lobes: left medial and lateral lobes, quadrate lobe, right medial and lateral lobes, and caudate lobe. Sonographically, the distinction between liver lobes is poorly defined. The left liver is largest and may comprise up to half of the liver mass. The gallbladder contacts the quadrate and right medial lobes. The left liver can be seen lateral and to the left of the gallbladder, and medial to the gastric fundus. The caudate process of the caudate lobe contacts the right kidney at the renal fossa (see Figure 8.1A,B). In general, it is difficult to visualize the divisions between liver lobes unless peritoneal fluid is present (see Figure 8.2E). Falciform fat can be imaged in the near‐field at the ventral liver margin (see Figures 8.2A–D, 8.10C and 39.2). A hyperechoic (bright white) line is imaged cranial to the liver. While this is commonly referred to as the diaphragm, it is actually the interface of the muscular soft tissue diaphragm and the gas‐filled lung (see Figure 8.2B–E). When this echogenic curvilinear interface is not present or there is interruption of the normal curvilinear continuity of the structure, then congenital or acquired diaphragmatic herniation should be ruled out (see Figure 8.2F,G).
Evaluation of the size of the liver is subjective and is poorly assessed with ultrasound due to variability in patient conformation. Hepatic size estimation is better evaluated on abdominal radiographs. Normal liver margins are sharp and not rounded (see Figure 8.2A,B,E).
Normal hepatic parenchyma is homogeneous and uniform in echogenicity with medium echotexture (coarser echotexture than the spleen) (see Figure 8.1C,D). Echogenicity is generally evaluated in comparison with falciform fat, the right renal cortex and spleen (see Figures 8.1A,B and 8.2A–D). Falciform fat must be distinguished from hepatic parenchyma and is generally isoechoic or hyperechoic to normal hepatic parenchyma (see Figure 8.2A–D and compare to Figure 8.10D), with a coarser echotexture. The liver is hypoechoic (darker) compared to spleen and the left liver can often easily be compared to the head of the spleen whereas the right liver is easily compared to the right kidney, which allows for comparisons at the same image field of view at the same depth, focus and gain (see Figure 8.1C,D). The liver is normally isoechoic to mildly hypoechoic and coarser in echotexture compared to the renal cortex (see Figure 8.1A,B). Subtle changes in echogenicity of the hepatic parenchyma can be difficult to appreciate for the novice sonographer. Using the split‐screen B‐mode function can be helpful for comparing liver, renal and splenic echogenicity comparisons at the same depth, focus, and gain when these organs cannot be imaged in the same frame on nonsplit‐screen B‐mode scanning.
Pearl:Remember the “SLiCK” pneumonic regarding canine echogenicity: the spleen (S) is hyperechoic (brighter) to liver (Li) which is slightly more hyperechoic (brighter) or isoechoic (same echogenicity) to the cortex of the kidney (CK). In the order of most to least echogenic, this spells “SLiCK.” For the feline, hepatic echogenicity is often compared to the adjacent falciform fat and the feline liver should be isoechoic to slightly hypoechoic to the falciform fat.
Evaluation of hepatic vasculature should generally be reserved for the more experienced sonographer. However, distension of the hepatic veins is fairly easy to identify and can be learned by the novice. Hepatic veins are distinguished from portal veins based on the echogenicity of the walls. Portal veins have bright echogenic walls whereas the walls of the hepatic veins are not visualized (see Figure 8.10A,B). The hepatic veins can be traced through the hepatic parenchyma to the caudal vena cava to confirm their identity. The caudal vena cava traverses the dorsal hepatic parenchyma slightly to the right of midline, and the hepatic veins empty into the cava near the diaphragm ( Figure 8.3A,B). See also Chapters 7, 20, 26, and 36.
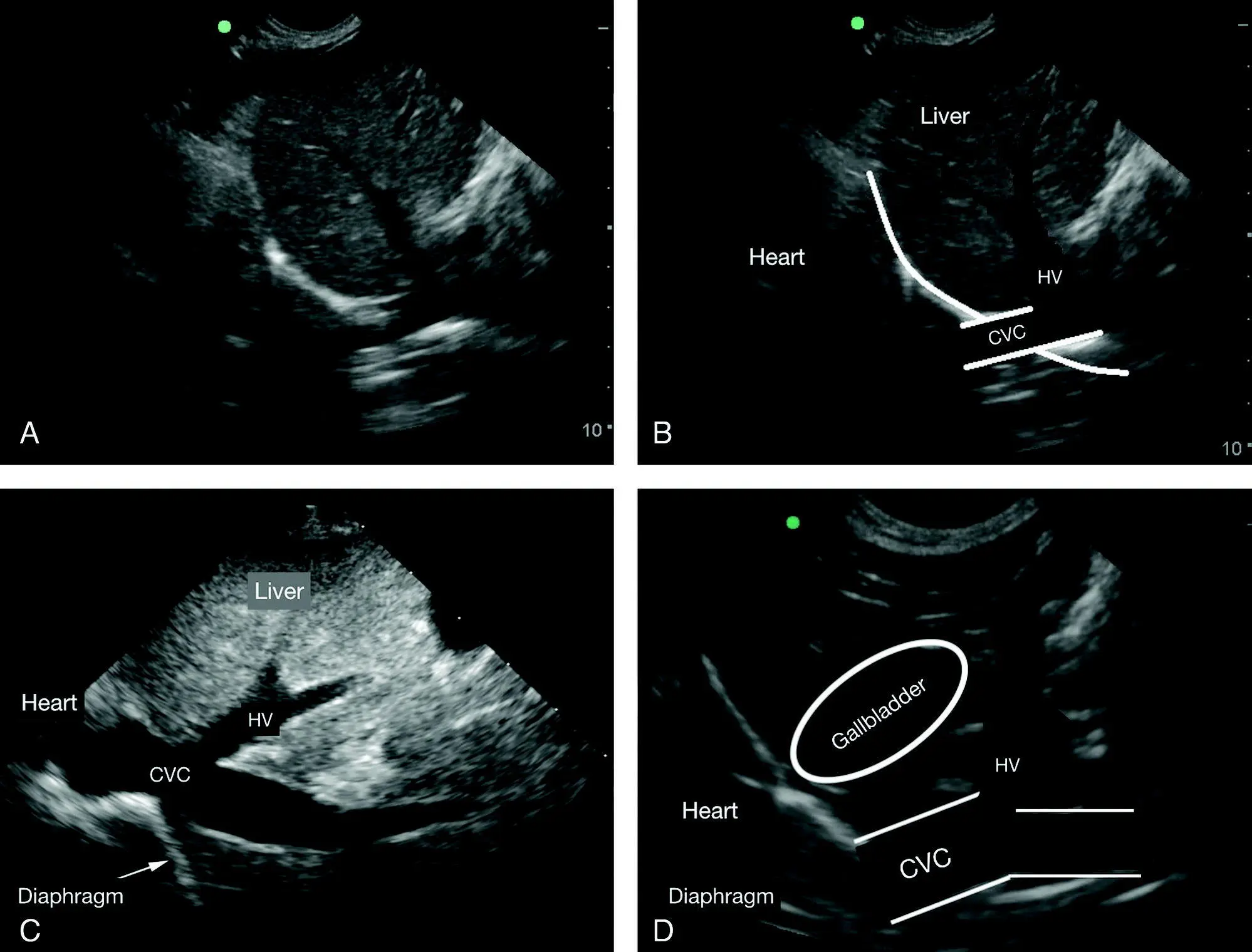
Figure 8.3. Hepatic venous congestion. The differentiation between hepatic veins and portal veins can be challenging for the novice. However, imaging the caudal vena cava as it passes through the diaphragm in the longitudinal plane is easy to learn and helps accurately identify distended hepatic veins by their associated branching into the caudal vena cava. Normally, hepatic veins are inconspicuous. Shown in (A) and (B) is the same example of moderate hepatic venous (HV) congestion unlabeled and labeled. Note how the hepatic veins can be seen emptying into the caudal vena cava (CVC) prior to the CVC passing through the diaphragm (Diaphragm →). The image was acquired at the TFAST diaphragmatico‐hepatic (DH) view. (C) Another example of HV congestion being traced to the caudal vena cava (CdVC) near the diaphragm (Diaphragm →). Detecting hepatic venous distension is clinically helpful and aids in the detection of right‐sided volume overload, right‐sided heart failure or an obstructive venous lesion between the liver and right atrium, which would then prompt further investigation and help guide management. (D) A similar correlative figure with overlays to show the anatomy of the area.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner»
Представляем Вашему вниманию похожие книги на «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.












Обсуждение, отзывы о книге «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.