Point-of-Care Ultrasound Techniques for the Small Animal Practitioner
Здесь есть возможность читать онлайн «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Point-of-Care Ultrasound Techniques for the Small Animal Practitioner
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Point-of-Care Ultrasound Techniques for the Small Animal Practitioner: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
New chapters in
cover ultrasound-guided nerve blocks, musculoskeletal, brain imaging, and applications of focused ultrasound techniques in cats, exotics and marine mammals—making it an essential purchase for veterinarians wanting to incorporate point-of-care ultrasound techniques into their veterinary practices.
Presents a standardized approach to point-of-care ultrasound as an extension of the physical exam, including trauma, non-trauma, and monitoring applications Includes coverage of new techniques for focused ultrasound exams, including lung, anesthesia and ultrasound guided nerve blocks, transcranial brain imaging, musculoskeletal, volume status evaluation, and rapid assessment for treatable forms of shock Adds cats, exotic and wildlife mammals, and marine mammals to the existing canine coverage Emphasizes the integration of point-of-care ultrasound techniques for optimizing patient care and accurate patient assessment Offers access to a companion website with supplementary video clips showing many clinically relevant didactic examples The second edition of
is an excellent resource for veterinary practitioners, ranging from the general practitioner to nearly all clinical specialists, including internal medicine, oncology, cardiology, emergency and critical care, anesthesiology, ophthalmology, exotics, and zoo medicine specialists, and veterinary students.
Point-of-Care Ultrasound Techniques for the Small Animal Practitioner — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Source: Reproduced with permission of Dr Gregory Lisciandro, Hill Country Veterinary Specialists and FASTVet.com, Spicewood, TX.
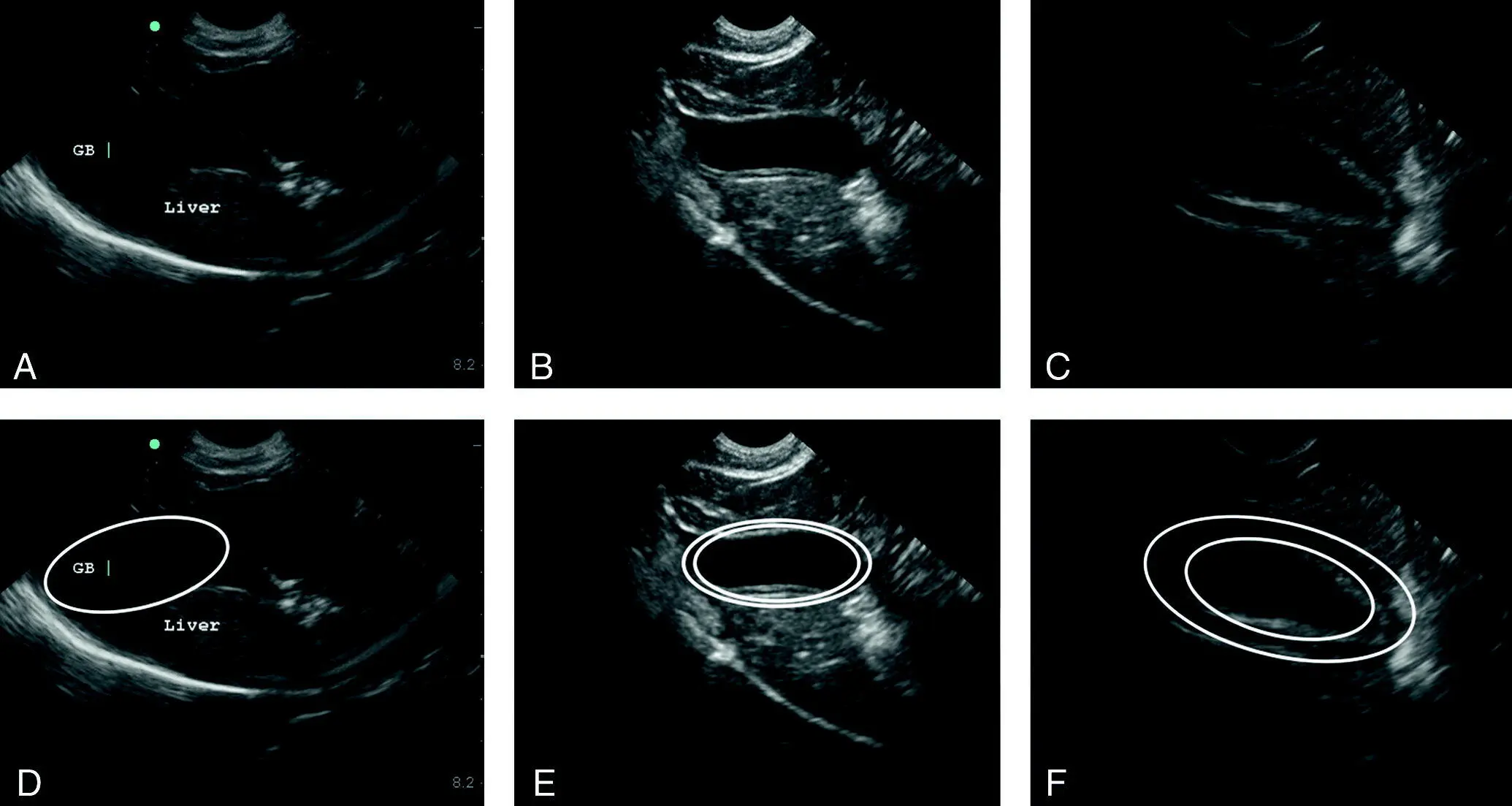
Figure 7.11. Gallbladder wall edema in dogs with anaphylaxis. Three different images with two different degrees of gallbladder wall edema in two different dogs at the AFAST DH view. Images in the top row are shown in the bottom row with correlating line drawing overlays. A normal gallbladder wall is for all intents and purposes a thin hyperechoic line as shown in (A) and (D). The gallbladder wall “halo effect” is in fact intramural edema that images as a hyperechoic inner wall, a hypoechoic or anechoic sonographic layer of intramural edema, followed by an outer hyperechoic wall. The sonographic striation, white‐black‐white or white‐gray‐white, is also referred to as the “halo sign” or “double rim effect” (Quantz et al. 2009). (B) and (E) is the same image unlabeled and labeled; note the small triangulations of free fluid (outlined with triangles), which would be scored as an AFS of ½. In (C) and (F) is another case with canine anaphylaxis with the same image unlabeled and labeled. The curved white line represents the diaphragm. Degrees of gallbladder wall edema in the author's experience do not correlate with severity of anaphylaxis. Gallbladder wall edema, although a marker for canine anaphylaxis, is not pathognomonic and PCE and right‐sided heart failure are major rule‐outs in the acutely collapsed or weak‐hypotensive dog (see Table 7.5and Figure 18.22).
Source: Reproduced with permission of Dr Gregory Lisciandro, Hill Country Veterinary Specialists and FASTVet.com, Spicewood, TX.
Table 7.5. Rule‐outs for the finding of gallbladder wall edema in dogs and cats.
Source: Reproduced with permission of Dr Gregory Lisciandro, Hill Country Veterinary Specialists and FASTVet.com, Spicewood, TX.
| Condition | Expected characterization of the caudal vena cava (CVC) | Speculated pathophysiology |
|---|---|---|
| Canine anaphylaxis a | Flat, hypovolemic CVC, (see Table 7.6) | Massive histamine release resulting in acute marked hepatic venous congestion |
| Pericardial effusion q | FAT, distended, hypervolemic CVC, referred to as vena cava plethora in people (see Table 7.6) (Himelman et al. 1988) | Marked hepatic venous congestion from obstruction of blood flow to the right atrium |
| Right‐sided congestive heart failure (dilated cardiomyopathy, pulmonary hypertension, tricuspid disease) a | FAT, distended, hypervolemic CVC, referred to as vena cava plethora in people (see Table 7.6) (Himelman et al. 1988) | Marked hepatic venous congestion from backflow of blood from the right atrium |
| Cholecystitis | Variable | Direct inflammation |
| Pancreatitis | Variable | Direct inflammation |
| Hypoproteinemia (third spacing) | Variable | Vascular leak |
| Immune‐mediated hemolytic anemia | Variable (author experience, unpublished) | Likely immune‐mediated and volume overload, does not indicate anaphylaxis in many patients |
| Post transfusion b | Variable to FAT, hypervolemia (author experience, unpublished) | Likely immune‐mediated and volume overload, does not indicate anaphylaxis in many patients |
aConditions that are most important to consider in the acute triage setting of acute collapse and weakness in a previously healthy patient (dog). FAT, flat, and bounce are defined in the text.
bMany posttransfusion cases develop gallbladder wall edema that is not anaphylaxis. Look at your patient and correlate its clinical profile with the finding of gallbladder wall edema.
Characterizing the Caudal Vena Cava
Measurements
Guidelines for caudal vena caval (CVC) absolute size in dogs of various weight classes have been created by the author from the data generously provided by Dr Elodie Darnis and colleagues (Darnis et al. 2018). More indepth CVC detail regarding measurements and formulas may be found in her co‐authored Chapter 26.
The expected CVC maximum heights for three weight classes of dogs taken in the longitudinal plane at the FAST DH view (subxiphoid) are shown in Table 7.6. The absolute height measurements should be combined with the “eyeball method” of evaluating respirophasic dynamic changes in the CVC. This gestalt “eyeball method” essentially assesses the CVC Collapsibility Index, which is the difference between maximum and minimum diameter divided by the maximum diameter multiplied by 100%.
The author has characterized the CVC as having a “bounce,” being “FAT” or “flat” for categorizing its clinical relevance to volume status. A “bounce” is a “fluid‐responsive” CVC; a “FAT” CVC is a distended CVC suggesting a “fluid‐intolerant” CVC reflective of an abnormally high central venous pressure (hypervolemia); and a “flat” CVC is a “fluid‐starved” CVC reflective of a “hypovolemic CVC.” The terms “FAT” and “flat” have been descriptively used in the human literature (Ferrada et al. 2012a,b) and many clinicians combine absolute maximum inferior vena cava height measurements with the “eyeball method” (FAT or flat). More and more, these same clinicians are incorporating basic echo views and lung ultrasound findings for more clinical integration to accurately assess volume status and thus guide fluid resuscitation in people (Ferrada et al. 2012a,b). Similar approaches are being investigated in veterinary medicine (Nelson et al. 2010; Lisciandro 2014a, 2016a, Lisciandro and Fosgate 2017; Bucci et al. 2017; Kwak et al. 2017; Tuplin et al. 2017; Darnis et al. 2018; Marshall et al. 2018; Cambournac et al. 2018) (see Chapters 26, 36, and 37and also Figures 36.8–36.12). The terms “FAT” (fluid intolerant, high central venous pressure, inferior vena cava >2 cm) and “flat” (fluid starved, low central venous pressure, hypovolemia) are routinely used in human medicine in the San Antonio area (Ferrada et al. 2012a,b). The author has added the term “bounce” for a fluid‐responsive CVC. The suggested CVC measurements shown in Table 7.6are at least a start and are easy to remember over formulas.
Table 7.6. Reference values for the caudal vena cava (CVC) measured in longitudinal at the subxiphoid aview in 126 healthy dogs, grouped into three body weight classes.
| Size | Body weight (kg) | Expected CVC height measurement (cm) | CVC +/‐2 standard deviations (cm) | Suggested CVC maximum height (cm) for a “flat” or hypovolemic, fluid‐starved CVC | Suggested CVC maximum height (cm) for a “FAT” or fluid‐intolerant CVC (high central venous pressure) |
|---|---|---|---|---|---|
| Small/Toy b | <9 kg | 0.55 | (0.23–0.86) | <0.25 | >1.0 |
| Medium | >9–15 kg | 0.85 | (0.32–1.38) | <0.35 | >1.5 |
| Large/Giant | >15 kg | 0.96 | (0.51–1.4) | <0.50 | >1.5 |
Data from the study by Darnis et al. (2018) and measurements created with permission by Lisciandro GR and Vientós‐Plotts AI. These values are unproven but give some guidelines for veterinary clinicians to combine with the eyeball method – “bounce”, “FAT,” and “flat.”
aThe subxiphoid view is analogous to the FAST DH view and the CVC imaged in its longitudinal plane.
bSuggested starting point for felines while awaiting current research findings.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner»
Представляем Вашему вниманию похожие книги на «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.












Обсуждение, отзывы о книге «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.