Jeffrey McCullough - Transfusion Medicine
Здесь есть возможность читать онлайн «Jeffrey McCullough - Transfusion Medicine» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Transfusion Medicine
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Transfusion Medicine: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Transfusion Medicine»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
The Fifth Edition of
delivers a succinct, thorough, clinically focused, practical and authoritative treatment of a full range of topics in transfusion therapy. This ranges from issues with the blood supply, recruitment of both whole blood and apheresis donors, blood collection and storage, blood testing, blood safety, and transmissible diseases. This edition has been fully updated and revised to include exciting cellular therapies for cancer, transplantation of both hematopoietic cells and solid organs, infectious diseases and regenerative medicine.
The Fifth Edition includes new authors with highly relevant content that provides a solid grounding for readers in the field. The book:
Is an approachable comprehensive guide to the field of blood banking and transfusion medicine Provides complete and timely perspective on crucial topics, including the HLA system in transfusion medicine and transplantation and quality programs in blood banking and transfusion medicine Is extensively referenced, making it simple for readers to conduct further research on the topics of interest to them Includes new chapters on pediatric transfusion medicine and pathogen reduction Has an expended chapter on patient blood management Provides extensive discussions of the clinical use of blood transfusion in a wide variety of clinical situations including recent development In the management of acute traumatic blood loss Provides updated information about blood groups and molecular testing making inroads into clinical practice along with discussions of laboratory detection of blood groups and provision of red cells Perfect for all those working in the field of blood banking, transfusion medicine and hematology or oncology and fellows in pathology, hematology, surgery and anesthesiology.
is a good introduction for technologists specializing in blood banking and non-medical personnel working in areas related to hematology and transfusion medicine. Transfusion Medicine will also earn a place in the libraries of practicing pathologists with responsibility for blood banks.
Transfusion Medicine — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Transfusion Medicine», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Terumo Trima Accel
The Trima Accel can be used for collection of platelets, plasma, or red cells in various combinations [27, 35–39] with a single‐needle technique. The Trima Accel takes about 51 minutes to produce 3.5 × 10 11platelets [27]. Platelets are leukoreduced using an in‐line chamber during the collection procedure. Red cells, platelets, and plasma collected using the Trima Accel have satisfactory in vitro characteristics, in vivo survivals, and in vivo clinical effectiveness [35–40].
Haemonetics Instruments
The Haemonetics system uses a disposable, transparent Lucite centrifuge bowl for blood separation [9]. After venipuncture is performed and the donor is connected to the instrument, the operator activates the instrument and blood is pumped from the donor into the centrifuge bowl ( Figure 6.2). Anticoagulant–citrate–dextrose anticoagulant is added to the blood as it leaves the donor. The centrifuge bowl spins at approximately 4,800 rpm and continuously separates the blood as it enters the bowl. When the volume of blood removed from the donor exceeds the capacity of the bowl, plasma begins to exit the bowl and is collected in a bag. The platelet/buffy coat layer accumulates at the top of the red cells, and as the bowl continues to fill, this layer moves toward the exit port. When the platelets—visible as a white band between the red cells and plasma—reach the exit port, a valve is activated, diverting the flow pathway into a separate bag, where the platelets are collected. When the platelets have been collected, the blood flow is stopped, the pumps reversed, and the plasma and red cells recombined and returned to the donor. This cycle of filling the centrifuge bowl is repeated several times to obtain the desired platelet yield.
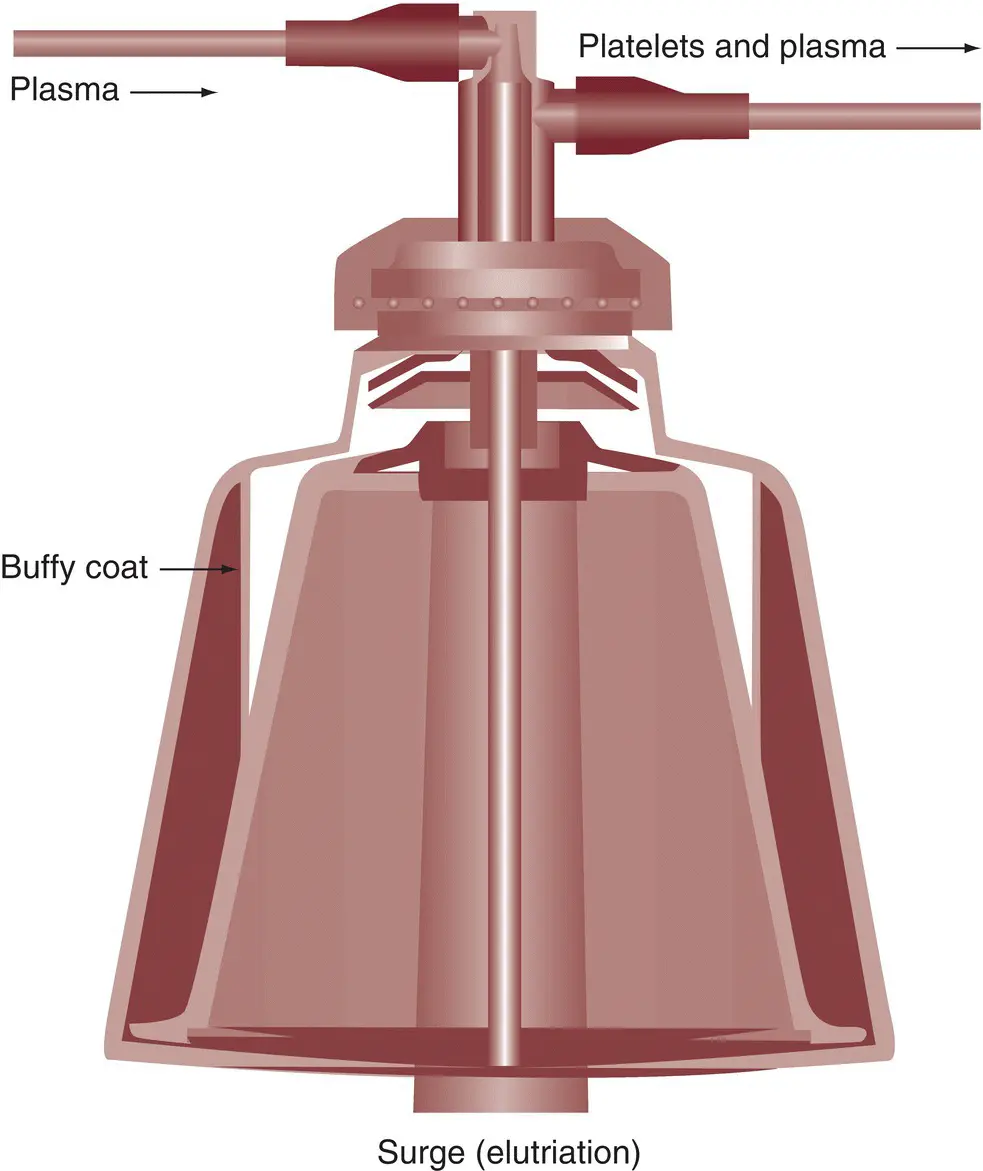
Figure 6.2 Flow pathway and blood separation in the Haemonetics Latham bowl system.
( Source : Courtesy of Haemonetics Corporation)
The Haemonetics Multiple Component Systems (MCS and MCS+) have the flexibility to collect various combinations of platelets, plasma, and red cells [41, 42] ( Table 6.1). The MCS and MCS+ can collect approximately 4 × 10 11platelets in 90 minutes [41, 42]. A combination of platelets and plasma can also be collected [43]. This exciting approach was finally the first step to provide flexibility to the donor center to determine on a daily basis or for individual donors the particular mix of components to collect.
6.2 Plateletpheresis
Single‐donor platelet concentrates
The official US Food and Drug Administration name of this component is platelets, pheresis. In daily practice, this component is usually called single‐donor platelets or plateletpheresis concentrates, a suspension of platelets in plasma or additive solution prepared by cytapheresis.
The use of apheresis, particularly for platelet production, is increasing substantially in many countries [44]. In 1982, about 80,000 plateletpheresis procedures were performed [45] in the United States, and by 2013, this had increased to 2,000,000 [46]. This accounted for about 90% of all platelets produced [46].
Platelets obtained by plateletpheresis are processed, tested, and labeled in a similar manner to whole blood (see Chapters 5and 7). This includes ABO and Rh typing and testing for all required transfusion‐transmitted diseases. The number of platelets contained in each concentrate is determined, although this information may not necessarily be recorded on the label. Each platelet concentrate has a volume of approximately 200 mL and contains very few red cells ( < 0.5 mL), and so red cell crossmatching is not necessary. Quality‐control tests must show that at least 90% of the apheresis platelet concentrates produced by each facility contain 3 × 10 11platelets or more [47]. The white blood cell (WBC) content varies depending on the instrument and technique used for collection, but presently all plateletpheresis procedures produce leukodepleted platelets ( < 1 × 10 6WBCs).
Function and storage of platelets obtained by apheresis
Platelets collected using these plateletpheresis systems have in vitro function and in vivo survival characteristics equal to platelets prepared from whole blood [10, 23, 36, 39, 48–52]. The platelets survived normally when autologous transfusions of radiolabeled platelets were given to normal research donors, and platelets collected by apheresis caused the expected increase in platelet count in patients with thrombocytopenia [36, 39, 53]. The preservation medium and the size and composition of the storage container make it possible to routinely store platelet concentrates produced by apheresis in a volume of about 200 mL for 5 days [54].
6.3 Erythrocytapheresis
Chronic shortages of certain types of red cells stimulated interest in the use of apheresis to collect the equivalent of two units of red cells from some donors, especially group O. Several instruments are now available for red cell apheresis [30, 31, 36, 38, 39, 55–60] ( Table 6.1). After removing RBCs, saline may be infused to the donor to maintain blood volume. The RBCs can be stored in an additive solution for the usual 42 days [30, 36, 39, 59]. The red cell products obtained by apheresis are much more standardized than red cells prepared from whole blood, but otherwise red cells obtained by apheresis have the same characteristics as those produced from whole blood ( Table 6.2). The advantages provided by red cell apheresis are to obtain two units of red cells from one donation to allow for fewer donor visits, possible increases in red cell availability, and potentially fewer donor exposures if both units of red cells from one donor are transfused to one patient.
Donors for two‐unit red cell apheresis must meet weight and hemoglobin standards specified for each instrument. Because two units of red cells are removed, they may donate only every 4 months. This is adequate for red cell recovery but may not allow complete regeneration of iron stores [61]. Apheresis for two‐unit red cell collection is taking its place in the mixture of blood component production activities ( Table 6.2). Although reactions following RBC collection by apheresis are more common than whole blood donation, almost all reactions were minor and for donors younger than 20 years, reactions are equally common after two RBC collections or a whole blood collection. Thus, two RBC collections are as safe as a whole blood collection [62].
Table 6.2 Comparison of red cell units prepared from whole blood with red cell units prepared by double‐unit red cell apheresis.
| Whole blood | Alyx a | Trima | MCS b | |
|---|---|---|---|---|
| Product volume (mL) | 310 | 301 | 347 | 312 |
| RBC volume (mL) | 190 | 177 | NA | 182 |
| Total hemoglobin (g) | 55 | 57.8 | 60.7 | — |
| Hematocrit (%) | 60 | 58 | 55 | 58 |
| Collection time (min) | 8 | 28 | NA | 50 |
NA, not available; RBC, red blood cell.
a Source : Louie J, Greco BJ, Martinez S. Quality and characteristics of red cells collected on a new automated portable component collection system. Transfusion 2003; 43(Suppl):135A (abstract).
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Transfusion Medicine»
Представляем Вашему вниманию похожие книги на «Transfusion Medicine» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Transfusion Medicine» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.