Salivary Gland Pathology
Здесь есть возможность читать онлайн «Salivary Gland Pathology» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Salivary Gland Pathology
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Salivary Gland Pathology: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Salivary Gland Pathology»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
now features case presentations to place the information in context, as well as additional treatment algorithms in each chapter to assist in clinical decision making. Written by highly respected clinicians, educators, and researchers with extensive expertise in oral and maxillofacial surgery, this authoritative resource:
Reviews the etiology, diagnosis, and treatment of all salivary gland pathologies, with detailed explanations and hundreds of full-color clinical images Incorporates new information on the taxonomy of salivary gland tumors, neoplastic and non-neoplastic entities, image guided biopsies of salivary gland lesions, and complications in traditional and non-traditional forms of salivary gland surgery Offers expanded coverage of histopathology, including classification, grading, and staging of salivary gland tumors Features up-to-date chapters on anatomy and physiology, imaging, cysts, systemic diseases, tumors, trauma, and innovative salivary gland surgical techniques Includes a discussion of meta-analyses and systematic reviews to support evidence-based practice remains the definitive resource for oral and maxillofacial surgeons, otolaryngologists, head and neck surgeons, and general surgeons as well as their residents providing care for patients with salivary gland pathology.
Salivary Gland Pathology — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Salivary Gland Pathology», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
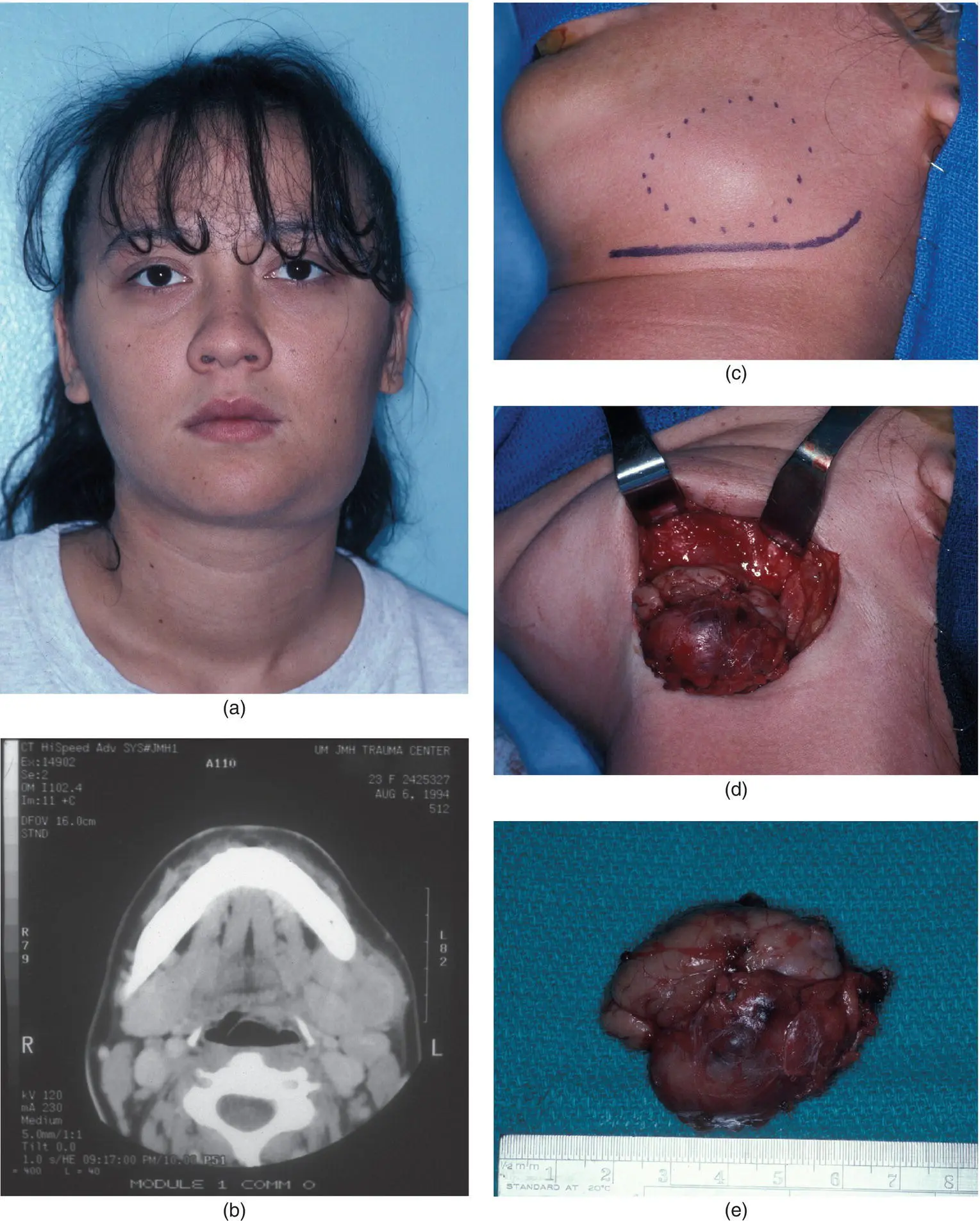
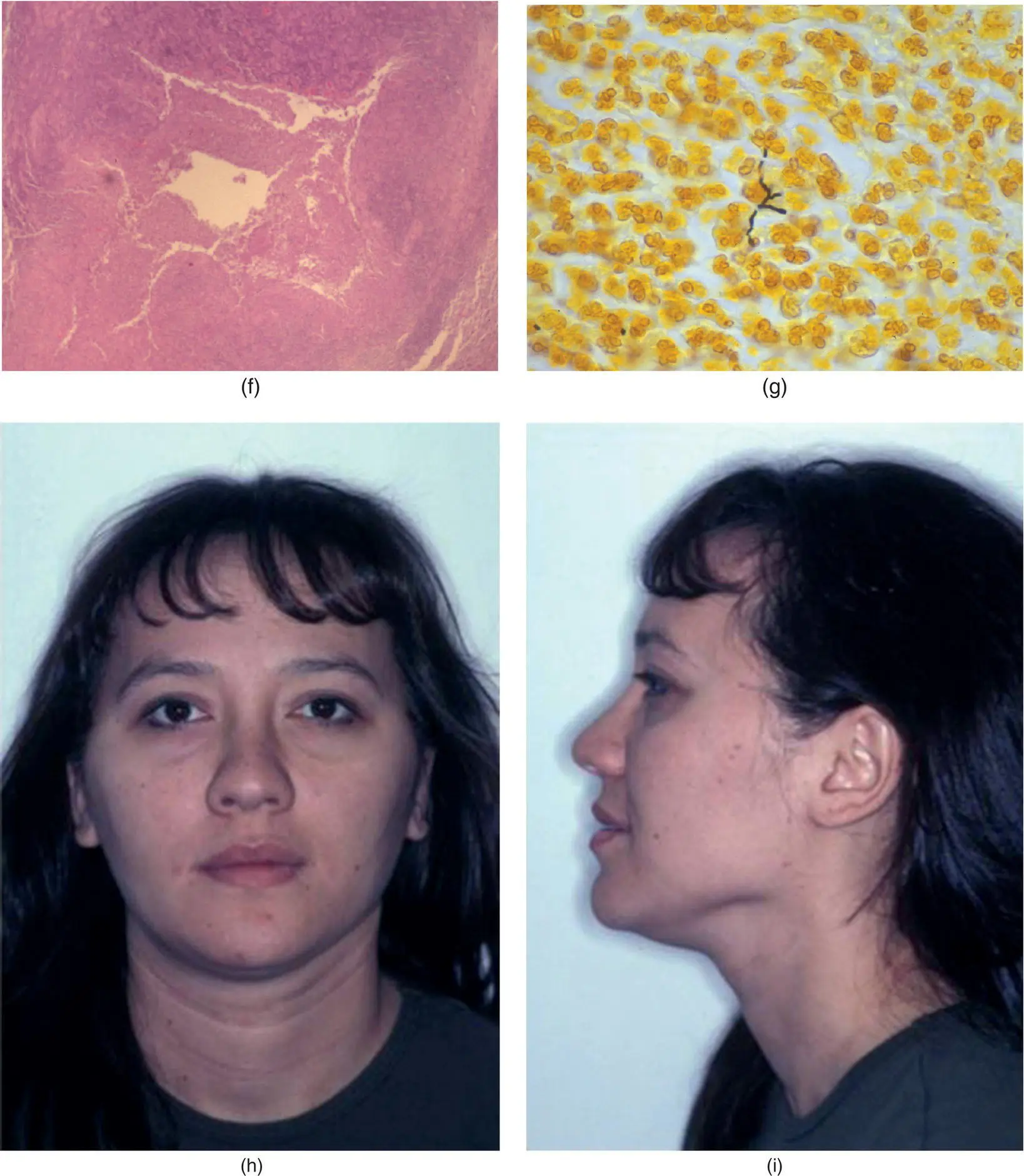
Figure 3.16. A 21‐year‐old woman (a) with a two‐week history of left submandibular pain and swelling. A history of animal scratch was provided. Computerized tomograms (b) revealed a mass of the left submandibular gland. The patient was taken to the operating room where excision of the submandibular gland and mass was performed. Wide access was afforded (c) and the mass was exposed (d). The specimen is noted in (e). Histopathology showed a stellate abscess (f). A Steiner stain (g) showed Bartonella (Gram negative bacillus). Her disease resolved without long‐term antibiotics as seen in five‐year postoperative images (h and i).
NONTUBERCULOUS MYCOBACTERIAL DISEASE
Nontuberculous mycobacterial disease has become an important entity in the pediatric population. It has been estimated that greater than 92% of mycobacterial cervicofacial infections in children are a result of nontuberculous mycobacteria (Arrieta and McCaffrey 2005). The disease primarily affects children younger than five years of age. The specific organisms are M. Kansasii, Mycobacterium avium‐intracellulare , and M. scrofulaceum . The typical clinical presentation is that of a rapidly enlarging and persistent parotid and/or neck mass that has failed to resolve with antibiotic therapy (Mitchell and Ord 1988) ( Figure 3.17). A characteristic violaceous discoloration to the skin develops. The treatment of choice is surgical removal of the involved salivary gland and associated lymph nodes.
Viral Salivary Gland Infections
MUMPS
Viral mumps is an acute, nonsuppurative communicable disease that often occurs in epidemics during the spring and winter months. The term mumps is derived from the Danish “mompen,” which refers to mumbling, thereby describing the difficulty with speech because of inflammation and trismus (McQuone 1999; Arrieta and McCafrey 2005). The nearly routine administration of the measles–mumps–rubella (MMR) vaccination has decreased the incidence of mumps in industrialized nations. Since the introduction of the live attenuated vaccine in the United States in 1967 and its administration as part of the MMR vaccine, the yearly incidence of mumps cases has declined from 76 to two cases per 100,000 (Murray et al. 1994). Mumps characteristically occurs in the parotid glands. Although the disease is typically seen in children between six and eight years of age, it may occur in adults who have avoided childhood infection, as well, and displays an equal sex predilection. The disease is caused most commonly by a paramyxovirus, a ribonucleic acid virus related to the influenza and parainfluenza virus groups. Several other nonparamyxoviruses may cause mumps, including coxsackie A and B viruses, Epstein‐Barr virus, influenza and parainfluenza viruses, enteric cytopathic human orphan (ECHO) virus, and human immunodeficiency virus (HIV). Mumps is transmitted by infected saliva and urine. The incubation period between exposure and the development of signs and symptoms is 15–18 days. A prodromal period occurs that lasts 24–48 hours and involves fever, chills, headache, and preauricular tenderness. Following the prodromal period, rapid and painful unilateral or bilateral swelling of the parotid glands occurs. Features that distinguish sialadenitis due to mumps versus bacteria include a lack of purulent discharge, positive serum titers for mumps, and a relative lymphocytosis in mumps. In addition, the clinical presentation of mumps is mild; not infrequently, patients may be asymptomatic (Schreiber and Hershman 2009). The diagnosis is made by demonstrating complement‐fixing soluble (S) antibodies to the nucleoprotein core of the virus, which are the earliest antibodies to appear. These antibodies peak at 10 days to 2 weeks and disappear within eight to nine months. The S antibodies are therefore associated with active infection. The complement‐fixing viral (V) antibodies are against outer surface hemagglutinin and appear later than S antibodies but persist at low levels for years. The diagnosis may also be made by isolating the virus from urine, which is possible up to 6 days prior and 13 days after the salivary gland symptoms occur (Rice 1998. Serum amylase levels may be elevated regardless of an associated pancreatitis. Abdominal pain is often indicative of mumps pancreatitis. Mumps orchitis occurs in 20% of adult males who have mumps parotitis (Goldberg and Bevilacqua 1995). Approximately half of these males will experience secondary testicular atrophy that may result in sterility if the testicular atrophy occurs bilaterally. Other rare complications of mumps include mumps hepatitis, mumps myocarditis, and mumps thyroiditis.
Treatment of mumps is supportive as spontaneous resolution of the disease occurs within 5–10 days. Such supportive care includes bed rest, proper hydration, and dietary modifications to minimize glandular activity. Persistent or recurrent parotid swelling may indicate the presence of sialadenitis. In the presence of such symptoms, a CT scan may be ordered that will frequently identify generalized sialadenitis to all salivary glands ( Figure 3.18).
HUMAN IMMUNODEFICIENCY VIRUS
HIV infection is associated with numerous pathologic processes involving the salivary glands, with the parotid gland being the most common. Parotid gland enlargement is estimated to occur in 1–10% of HIV‐infected patients (Shanti and Aziz 2009). HIV‐associated salivary gland disease (HIV‐SGD) is a term used to describe the diffuse enlargement of the salivary glands. HIV‐SGD may affect patients throughout all stages of the infection, and may be the initial manifestation of HIV infection (Schiodt et al. 1992).
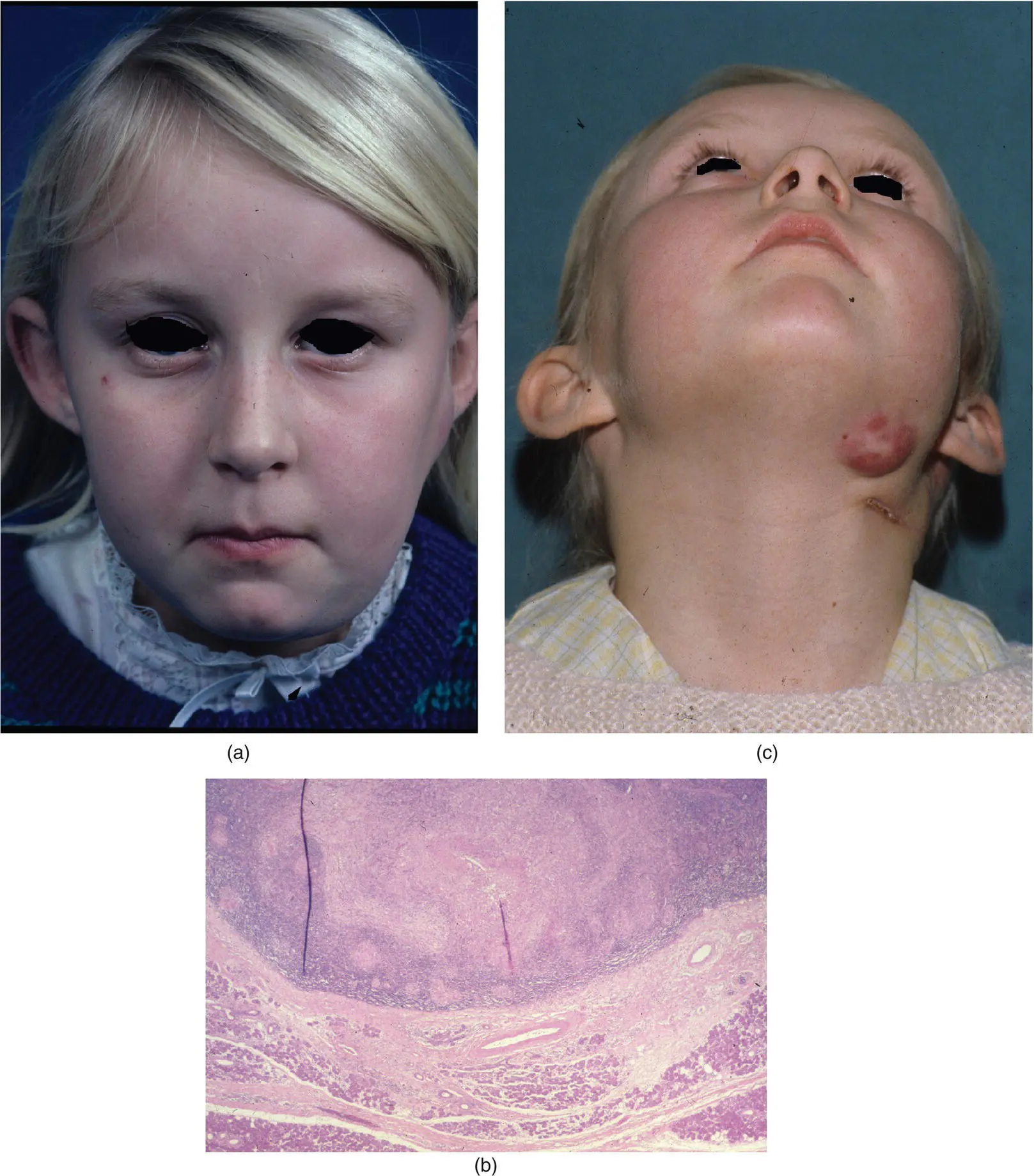
Figure 3.17. A 9‐year‐old girl with a left parotid swelling with overlying erythema of skin but no signs of acute infection (a). The patient underwent left superficial parotidectomy and excision of a submandibular lymph node. Histopathology showed noncaseating granulomas (b), and cultures showed mycobacterium avium‐intracellulare. Two months following the parotidectomy, a left submandibular lymph node became enlarged (c) and was treated with medical therapy.
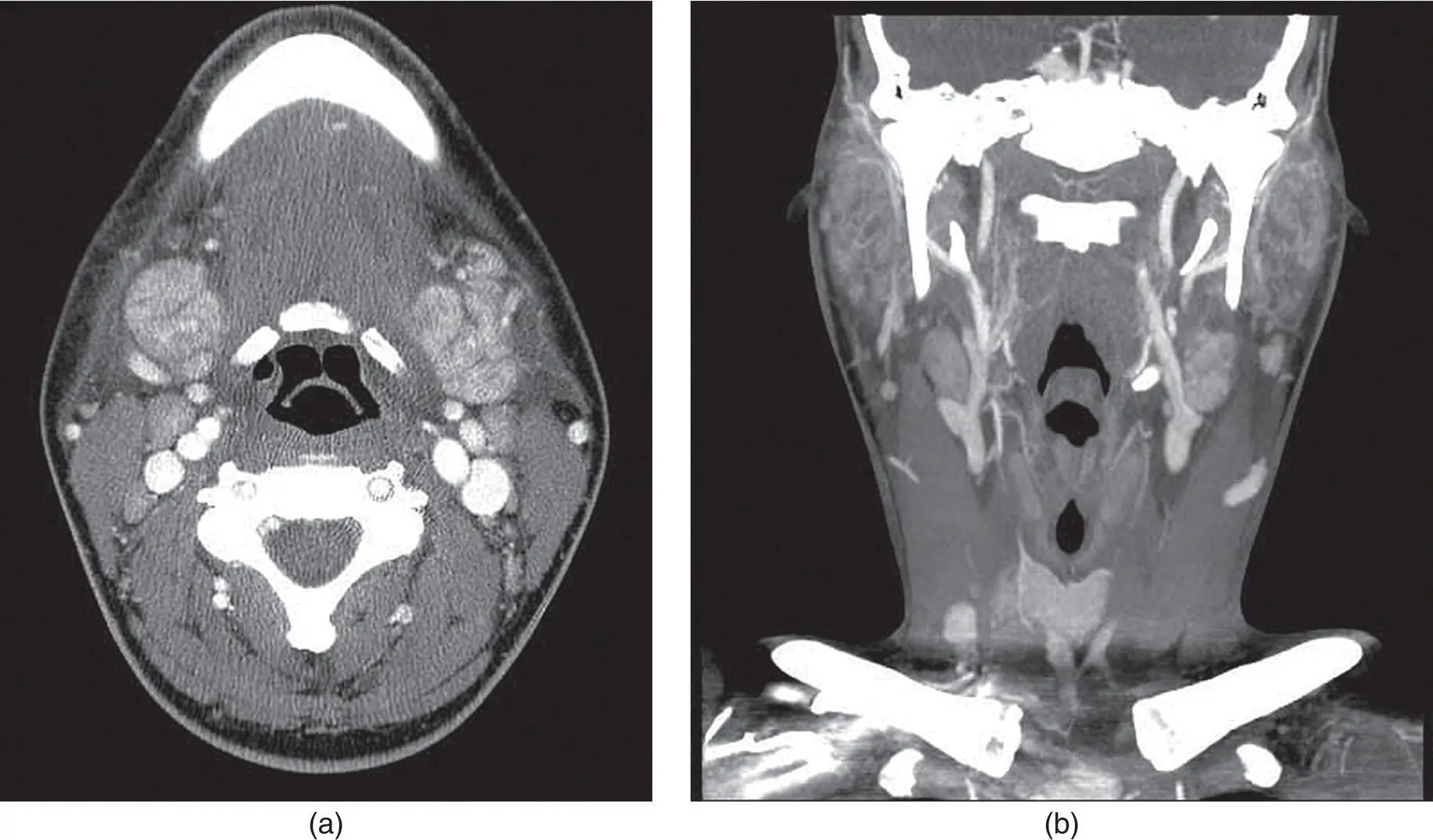
Figure 3.18. Axial (a) and coronal (b) CT images demonstrating contrast enhancement of bilateral submandibular and parotid glands in a patient with a clinical viral prodrome.
Patients with HIV‐SGD present with a history of nontender swelling of one or more of the salivary glands ( Figure 3.19). These swellings may fluctuate, but are generally persistent. Imaging studies are generally beneficial to diagnose lymphoepithelial cysts in this patient population that may clinically resemble the nontender swellings of the parotid glands in this patient population. Decreased salivary gland function results in xerostomia and sicca symptoms. This sicca symptom complex mimics Sjögren syndrome and has resulted in the classification of another HIV‐related salivary gland process known as the diffuse infiltrative lymphocytosis syndrome (DILS). This pathologic process is characterized by the presence of persistent circulating CD8 lymphocytes and infiltration of organs by CD8 lymphocytes that occur predominantly in the salivary glands and lungs. While DILS appears clinically like Sjögren syndrome, it can be differentiated by the presence of extraglandular involvement of the lungs, kidneys, and gastrointestinal tract. In addition, Sjogren's autoantibodies will be absent in patients with DILS.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Salivary Gland Pathology»
Представляем Вашему вниманию похожие книги на «Salivary Gland Pathology» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.








Обсуждение, отзывы о книге «Salivary Gland Pathology» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.