Paul Coceancig - 6Ways to Design a Face
Здесь есть возможность читать онлайн «Paul Coceancig - 6Ways to Design a Face» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:6Ways to Design a Face
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
6Ways to Design a Face: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «6Ways to Design a Face»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
6Ways to Design a Face — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «6Ways to Design a Face», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
This book is in effect a chronicle of those ideas and their assimilation into a complex philosophy and then a practical set of new operations and new treatments. My six ways to design a face include IMDO, GenioPaully, custom BIMAX, SuperBIMAX, custom PEEK, and SARME. I am not the inventor of any of these things. The appearance of their originality is a silk screen, behind which lies an indescribably complex history and the serial and compounded efforts and stories of millions of people.
It is unimaginable to me that any person would willingly submit themselves to any of these operations, however simple or complex. Although I have always acted gently and hopefully painlessly, and with compassion and with precision, it is another level completely to trust themselves to be the first to an operation never before performed, let alone believed. So I’d like to thank the patients whose stories illustrate this book. If there is an inventor, it was the individual child who would suggest to me that their condition was curable.
If only I would become as imaginative as their own mind in describing their own condition, and a match to their inspirational hope.
1
REIMAGINING ORTHODONTICS AND ORAL SURGERY
History should never be ignored, but it always is. In every clinical discipline, fundamental premises or truths exist to drive the culture, practice, and scientific enterprise of that specific clinical group. History establishes how one thought or practice began and of course leads to another and the next. Through history we see why we do things a certain way today. It is in history that we see how our forebears interpreted the same observations we still see, and how their older philosophies of care underpin our modern clinical practices and wider community expectation.
Not all clinical disciplines are necessarily in agreement with each other. Chiropractors, osteopaths, and naturopaths undoubtedly disagree with physicians over many things. But no matter their underpinnings (respective of philosophical or scientific premise), almost all clinical groups were initially founded by a single person (or guru or saint). And yet we pretend that because we live in today, that it specifically equates to modernness or betterness, and what was in the past—which is by default old or ancient—has no part to play in how we think or practice today.
Our modern disciplines have evolved to be rooted only in new science, eternal debate, and collective polite argument. We can only accuse the other distant craft group of quackery. As proper scientific doctors we simply cannot believe that deception and magic and nonscience and esotericism can exist in ourselves. But is there really any true separation of modern practice from older practice? Are our modern treatments really so different to our founding fathers’ so many centuries or decades or years ago? Are we really doing so much better? Consider Fig 1-1.
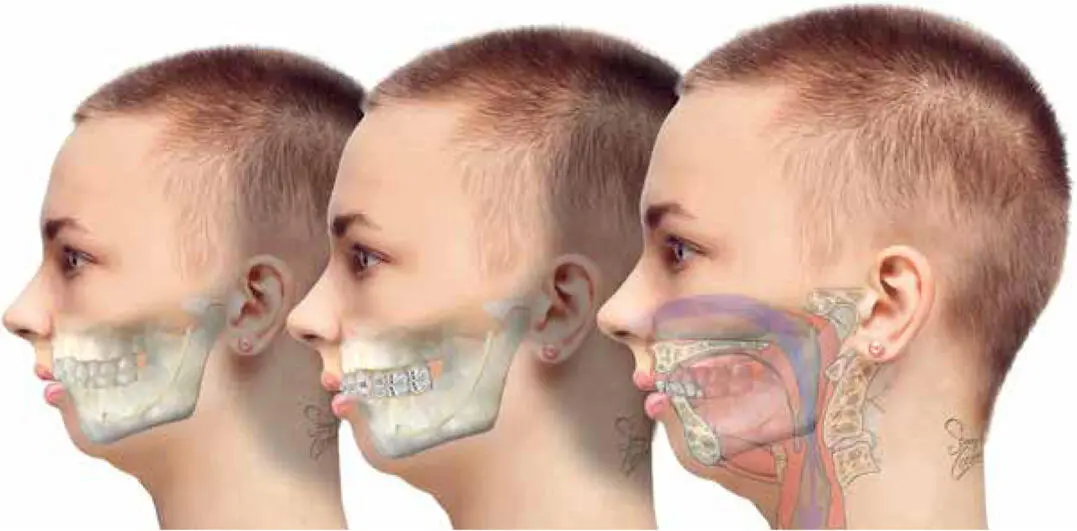
FIG 1-1 Traditional orthodontics alone with dental extractions and removal of impacted third molars will result in straight anterior teeth, but this century-old, well-established, and universally accepted treatment ignores the why and how of tooth crowding, as well as how the airways, face, tongue, jaws, and teeth are all indivisibly interrelated.
ORTHODONTIC DIAGNOSIS
Orthodontics was largely introduced by Edward Angle in 1895. He described the classification of “malocclusion”—a Latinization he invented to describe a “bad bite”—as Class I, Class II (division 1 or 2), or Class III. Orthodontists today still use the Angle classification of malocclusion to “diagnose” orthodontic cases, adding words such as “mild” or “severe” to further describe these classes followed by other descriptors such as “redundant” or “impacted” teeth or incisor relationship or jaw-profile association.
In the context of a purely dental clinical examination, a 12-year-old child with prominent maxillary anterior teeth may be described as a “severe Class II bilateral molar malocclusion, with significant incisor overjet, deep incisor overbite, and moderate mandibular incisor crowding, with impacted maxillary canines and impending third molar impactions” (see Fig 1-2).

FIG 1-2 Severe dental crowding in a 12-year-old as seen on a panoramic radiograph. In a “normal” 12- to 13-year-old, without considering the third molars, the 28 permanent teeth should all erupt into a Class I occlusion, and there should be no retained primary teeth. Multiple impacted canines and second molars and impending impacted third molars can be orthodontically seen as a dental state of “late eruptive development” or of “premolar or third molar redundancy” or simply as “too many teeth.” By contrast, the maxillofacial surgeon’s view is to see that there is a normal developing complement of 32 adult teeth, there is a primary smallness of the jaws, there are codeveloping facial and airway problems, and all of it can only formally be evaluated by total-head 3D head analysis, or via volumetric medical CT imaging.
Further dental analysis can be given with lateral cephalometry ( Fig 1-3). The measurements of angles and proportions of certain points and positions of the facial bones and skull base began in the late 19th century, alongside the science of anthropometry, which eventually incorporated radiographic imaging in the early 20th century. The language of modern cephalometry is orthodontically oriented. It has its own culture bred from a hundred different voices with racially separated data sets identifying what is “normal” and “abnormal.” It exists only for orthodontists and today is rarely used by jaw correction surgeons.

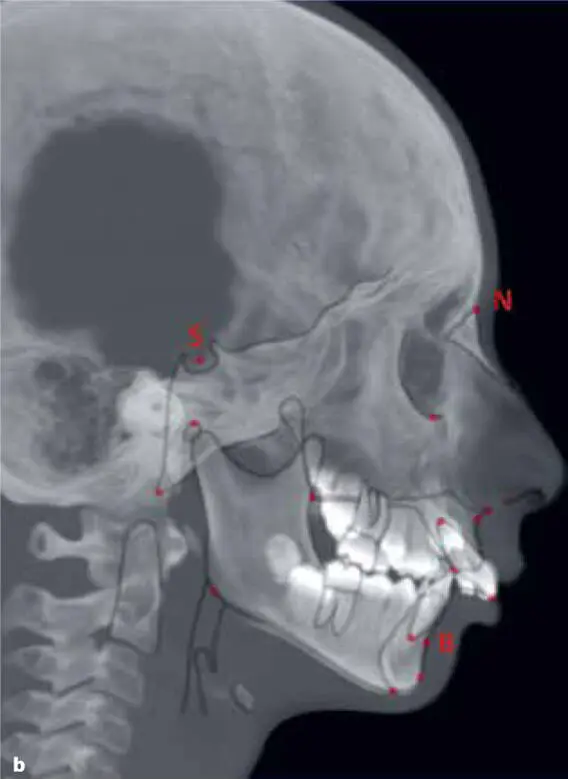
FIG 1-3 (a and b) An assessment of the profile of the same 12-year-old child with prominent maxillary anterior teeth may now include an orthodontic description of the jaw base. The cephalometric analysis evolves the orthodontic diagnosis as “severe Class II bilateral molar malocclusion, with significant incisor overjet, deep incisor overbite, and moderate mandibular incisor crowding, with impacted maxillary canines and impending second and third molar impactions, on a platform of anterior maxillary excess shown by excessive SNA angle and mild SNB angle deficiency.” While the airway can be imagined on a lateral cephalogram, it is often poorly seen. Inherent postures such as neck uprightness and unnatural head position coupled with the awake state as well as transient states such as breath holding, swallowing, jaw posturing, general movement, and lip pursing, not to mention the general anxiety of the child entering the x-ray machine, all affect how the soft tissues tense and move as well as how reliably they can be interpreted or referenced. In my view, which is supported by meta-analysis, 1the best measurement to determine whether a mandible truly lengthens due to an interventional orthodontic or surgical mandibular treatment is to compare the SNB angle on serial lateral cephalometry. Measuring changes in the SNB angle is relatively free of the confounder of growth and is not affected by genioplasty or GenioPaully. An accurate SNB measurement requires that the child does not posture the jaw forward—a notoriously difficult thing, as natural jaw joint position on lateral cephalometry is extremely difficult to confirm. The full treatment for this case is presented in chapter 9, along with our method of validating her surgical outcomes.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «6Ways to Design a Face»
Представляем Вашему вниманию похожие книги на «6Ways to Design a Face» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.



Обсуждение, отзывы о книге «6Ways to Design a Face» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.