Bone and Soft Tissue Augmentation in Implantology
Здесь есть возможность читать онлайн «Bone and Soft Tissue Augmentation in Implantology» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Bone and Soft Tissue Augmentation in Implantology
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Bone and Soft Tissue Augmentation in Implantology: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Bone and Soft Tissue Augmentation in Implantology»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
R. Gruber, Th. Hanser, Ph. Keeve, Ch. Khoury, J. Neugebauer, J. E. Zöller
Bone and Soft Tissue Augmentation in Implantology addresses useful methods of bone grafting procedures in implant treatment based on current biologic principles and constitutes a unique reference in this field. The book describes, in over 760 pages and 2837 mostly color illustrations, the different possibilities available to augment the bone volume in width and height. The information presented includes not only the underlying scientific concepts of the different augmentation techniques with autogenous bone, but also the associated soft tissue management, from safe approaches to different possibilities for soft tissue augmentation and papilla reconstruction techniques.
The book provides surgeons with a basic understanding of the biologic response to bone grafting procedures. Experienced implantologists will benefit from the in-depth background information, details of high-level surgical techniques, and scientific results, which will enable them to optimize their surgical procedures. Each chapter offers a wealth of information on the specific topic covered, with much attention given to the scientific concepts behind each one. Extensive case reports with step-by-step documentation allow readers to gain an impression of what is possible today in the 3D reconstruction procedures of the alveolar crest. Important criteria for success are presented as well as possible complications and their treatment.
Bone and Soft Tissue Augmentation in Implantology is a must-read for every implantologist, oral and maxillofacial surgeon, and any dentist interested in surgery.
Bone and Soft Tissue Augmentation in Implantology — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Bone and Soft Tissue Augmentation in Implantology», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
When using traditional periapical radiographs, the parallel technique is metrically more accurate than the half-angle technique. 73The use of a holder system for the parallel technique allows for secure positioning, so that a true-to-size and precise image recording can be achieved. Nevertheless, this may lead to deviations or distortions. Therefore, length determination should be verified by an earlier (already created) panoramic radiograph or CBCT in order to achieve an accurate length determination for implant planning.
Use of the dental status for extensive planning has not proven to be successful because the spatial relationships can only be insufficiently detected and there is the risk of an incorrect assessment of the vertical dimension due to deviations in the projection technique. Limited information regarding bone quality can be determined by a periapical radiograph.
Implant therapy is long term and requires appropriate follow-up assessments to evaluate the individual risk of peri-implantitis. Therefore, in addition to the initial diagnosis for the planning of the surgical procedure, the documentation of findings for the completion of the prosthetic restoration is also important. It is essential that these are available later on in the course of treatment. Especially for the evaluation of the crestal bone level of the individual implants, periapical radiographs still show the highest information density today. Digital archiving allows for a comparison of several images on the screen to assess, for example, the development of the peri-implant bone level.
Panoramic radiographs
The panoramic radiograph is an overview, giving general information on the dentition and bone volume and allowing the localization of anatomically sensitive structures such as the inferior alveolar nerve, sinus floor, and nose. Panoramic radiographs show an enlargement of 15% to 25% of the anatomical structures; this varies between the different company brands and also depends on the positioning of the patient during the scan. In the case of implant planning in the proximity of anatomically relevant structures, a reference ball is positioned per segment in order to obtain the most accurate metric analysis possible in the surgical field ( Fig 2-14c). With the aid of tomography, rough information regarding the bone quality is provided. Additional devices also provide transversal layers of the planned operating area, first made possible by the Scanora device. 5However, since these layers have to be controlled individually, no data can be created for further processing in planning and surgical guide software. One of the latest developments is panoramic imaging using the multilayer technique. During a standard scan, about 4000 raw images are stored, which also allows for a repeated reconstruction to change the position of the skull or the size of the panoramic curve. Due to the multiple slices, the visualization of the bone structures is improved, which offers more information about the expected bone quality.
For planning implants in routine cases or in cases with moderate atrophy, the panoramic overview provides very good information about the positional relationships, so that usually no further radiologic diagnosis for implant positioning is necessary.
Skull radiographs
In the semi-axial skull radiograph pa (posterior– anterior beam direction), the skull is partially imaged and, when correctly positioned, allows for the superimposed representation of the zygomatic bone and the maxillary sinus. This image allows for the evaluation of the transverse extent of the antrum. In addition, in a side-by-side comparison, it provides information on the presence of foreign bodies or any sinus pathology. The image is taken at maximum mouth opening, whereby the horizontally guided central x-ray beam enters about 10 cm above the external occipital protuberance and leaves the skull at the spina nasalis ( Fig 2-15).
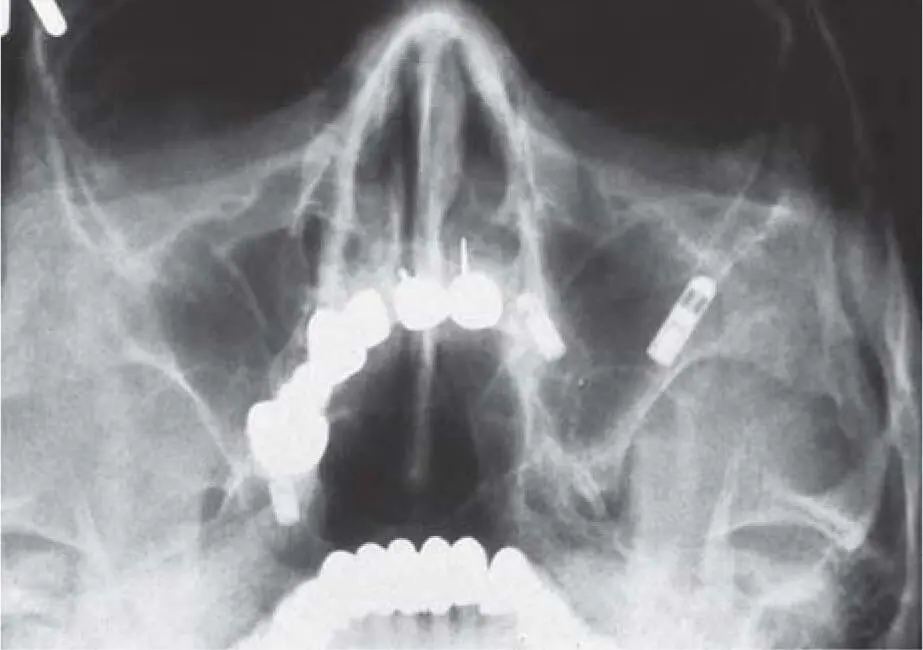
Fig 2-15Paranasal sinus radiograph with an implant in the maxillary left sinus.
Lateral skull imaging with a laterocentral beam through the sellar region is used at a distance of > 1.5 m as a lateral cephalogram, essentially for cephalometry in orthodontic treatment. For implant planning, this image can impart important information about the sagittal position of the maxilla and mandible as well as the inclination of the incisors and the orientation of the anterior ridge. By showing the contour of the removable prosthesis with tin foil, the degree of atrophy in relation to the necessary prosthetic reconstruction can be determined.
When bone harvesting from the chin is planned, this type of radiograph is useful to preoperatively determine the form and volume of the bone in the symphysis area as well as the amount of bone healing that occurs postoperatively ( Fig 2-16ato c).

Fig 2-16aCephalometric radiograph for determining the available bone in the chin area: progenic position of the mandible due to the atrophy of the maxilla.

Fig 2-16bControl radiograph after implant placement and bone harvesting from the chin area, which was covered with a titanium membrane (see also Chapter 4). Due to the grafting of the maxilla and the implant placement in the mandible, the sagittal step could be significantly reduced.

Fig 2-16cControl image 10 years postoperatively with well-regenerated donor site.
Computed tomography
In medical hard tissue diagnosis, computer tomography (CT) is the gold standard for three-dimensional (3D) imaging. Medical CT offers 3D imaging that allows for a distortion-free, metrically correct spatial diagnosis and planning, including the anatomical structures. If the CT scan is performed with a radiopaque setup of the prosthetic wax-up, the implant planning can even be performed from a prosthetic point of view. In CT, the x-ray beam is picked up by a line-shaped detector, the layers being obtained by rotating the radiation source and the detector around the patient. In the initial CT, the patient is pushed further through the gantry, so that the number of slices and the distance of the scan determine its resolution. 39
Today, a continuous feed generates a 3D volume on spiral CTs, which is then visualized in layers. Various protocols exist for performing a low-dose scan to reduce the primary dose. 91For medical indications, the visualization of hard- and low-contrast structures (soft tissue) is important. Therefore, a high energy is necessary, which limits it for routine use in the dental office.
Due to the scattered radiation caused by metallic prosthetic structures, it is important to position the patient carefully, depending on whether one is scanning the maxilla or mandible, so that the jaw can be aligned parallel to the beam path. If the patient is not properly positioned, metal scattering may limit the diagnostic value of the image in determining anatomical structures. Extensive prosthetic restorative reconstructions, such as a fixed partial prosthesis made of zirconia ceramic, may impair the diagnostic accuracy due to scattered radiation. By altering the gantry inclination of the spiral CT scan, the direction of the metal scatter can be changed, resulting in the improved usability of the scan. However, this requires a well-trained radiologist who is familiar with dental details. Due to the high initial cost and the fact that a radiologist is required to take the scan, this diagnostic tool is offered exclusively in centers for radiology ( Fig 2-17aand b).
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Bone and Soft Tissue Augmentation in Implantology»
Представляем Вашему вниманию похожие книги на «Bone and Soft Tissue Augmentation in Implantology» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Bone and Soft Tissue Augmentation in Implantology» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.