Adrian Becker - Orthodontic Treatment of Impacted Teeth
Здесь есть возможность читать онлайн «Adrian Becker - Orthodontic Treatment of Impacted Teeth» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Orthodontic Treatment of Impacted Teeth
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Orthodontic Treatment of Impacted Teeth: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Orthodontic Treatment of Impacted Teeth»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Provides protocols for common cases as well as complex and rare presentations Contains individual chapters on the specific aspects of the diagnosis and treatment of impaction in each of the different types of teeth Covers prevalence, etiology, diagnosis, attitudes to treatment, treatment timing, treatment methods, and prognosis Features more than 1,000 high-quality color images and illustrations
remains essential reading for all specialist orthodontists, academic researchers and instructors, oral and maxillofacial surgeons, and advanced students in orthodontics.
Orthodontic Treatment of Impacted Teeth — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Orthodontic Treatment of Impacted Teeth», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
It is the orthodontist’s main duty to try to create conditions that will replicate this natural eruption process as closely as possible. Accordingly, the practitioner will need to treat the follicle conservatively. If the follicular tissue is totally removed, a gingival attachment direct to the enamel of the crown of the tooth can no longer be expected to succeed. Indeed, the attachment that will result will be on cementum, at the root surface or somewhere below and beyond the CEJ. The unfortunate result will then be an elongated clinical crown and a compromised periodontal result ( Figure 5.9).
In the case of the surgical extraction of an impacted wisdom tooth, it is essential to carefully dissect out the dental follicle. This will prevent the possible later occurrence of cysts that may form from residual follicle epithelium. It follows that, in the absence of the wisdom tooth, the residual follicle has no function, other than its potential nuisance value. This, however, is not the case when the wisdom tooth is exposed and not extracted. In this latter situation, the surrounding follicle has an important function to fulfil – a function that is identical to the function of a normally erupting tooth and is integral to the establishment of a normal biological support system. It is important to understand this essential difference between extraction and exposure of the wisdom tooth.
It has been demonstrated in regard to teeth that have been buried for a long period that pathological changes occur in the follicle surrounding the crown (see Figure 6.13). These changes will have brought the enamel surface into direct contact with the surrounding tissues [47]. It is easy to draw a parallel between this condition and the artificial environment produced by an impacted tooth, which has been surgically exposed and which, in the absence of extrusive force being applied, has subsequently become re‐buried in the tissues. If, for whatever reason, the tooth does not erupt spontaneously, a long‐term direct contact between the tissues and the enamel of the tooth will occur.
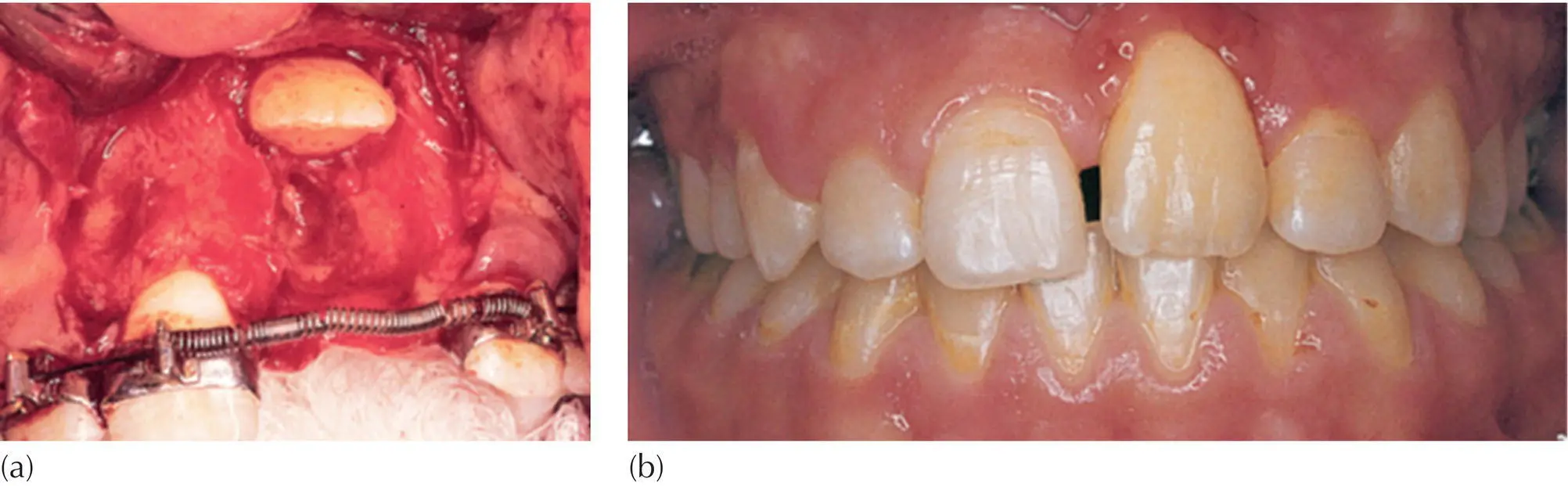
Fig. 5.9 A case treated by the author in the mid‐1970s, before the era of the acid‐etch technique. (a) A left impacted maxillary central incisor had been exposed and the entire follicular sac removed, prior to cementing a band. (b) At two years post treatment, the gingival contour is poor, the clinical crown is long and there has been positional relapse of the previously aligned tooth.
The surgeon will need to make an opening, adequate in size and one that will not eventually close over, and will therefore work to clear the tissues surrounding an impacted tooth. In doing so, in general, the surgeon will deliberately and completely remove the follicle surrounding the tooth ( Figure 5.9). The oral epithelium will grow down the sides of the opening and into the area that has been surgically cleared of follicular tissue. It will grow down as far as the deepest point where instrumentation has occurred, which in this case will be at least to the CEJ or possibly a little way down the root surface. The depth of its descent will be entirely dependent on how carefully the surgery was performed. Such a depth is considerably more apical than one would expect to find in a tooth whose recent eruption has occurred spontaneously. A compromised gingival attachment will result. The subsequently erupted tooth will have a longer clinical crown and reduced alveolar crest height, in sharp contrast to a tooth that has erupted normally.
A new look must be taken at the surgical plan for the exposure of unerupted teeth. If bonding will not take place during the surgical procedure, then, in order to prevent the re‐closing of the wound, a wider exposure must be performed and a surgical pack may need to be placed. Despite the importance of avoiding over‐zealous surgical removal of the follicle and of damaging the CEJ area by the forceful placement of the pack, a poorer periodontal result is to be expected. Attachment bonding will need to be performed as soon as convenient, subsequent to the removal of the pack. However, at such a later date, the healing and swollen gingival tissue surrounding the exposed tooth will be tender and will be covered with plaque that will have accumulated since the procedure. It will also bleed with minimum provocation, since effective tooth brushing in this delicate and sensitive area is unlikely to have been possible. These are not conditions that are conducive to reliable attachment bonding, despite the ease of access.
A wide flap design has the advantage of exposing the area of bone covering the tooth, and this will be helpful in identification of the exact site of the tooth. A canine tooth, buried in a bony crypt in the palate, will alter the shape of the palate inferiorly, by creating a distinct bulge of thinned bone that will be all the more obvious if a larger area of the surrounding bone is visible. The creation of a similar bulge is also the case in both the labial plate of the maxilla and in the buccal or lingual plate of the mandible. In order to avoid contamination with blood during bonding, distancing of the edges and underside of the flap from the field of operation is most important and is most easily performed when the flap design is generous.
Once the bony surface has been exposed and the location of the buried tooth identified, the thin overlying bone may be lifted off very easily. The surgeon will generally use a sharp chisel with light hand pressure to cut open the bony crypt and remove the superficial part of its wall. In some cases the bone may be paper thin and can be cut with a sharp scalpel. Immediately beneath the bone, the dental follicle will appear to glisten in the beam of the operating lamp. A window should be cut in the follicle to match the full extent of the very minimal bony opening that has already been achieved. This will enable a view of the orientation of the tooth as it lies in its crypt.
As we shall describe in later chapters, it is of utmost importance to place the orthodontic attachment as close as possible both to the mid‐buccal position of the crown of the tooth and to the incisal edge or cusp tip. This will ensure that the traction towards its place in the arch will tend to reduce any existing rotation and will reduce the amount of mechano‐therapy to which the tooth will need to be subjected. For this reason, where a rotated tooth is exposed, the bony opening should be extended around the crown of the tooth, towards the mid‐buccal area of the crown (provided that this can be done easily), while limiting further surgical damage. In this example, flap replacement may be completed and the pigtail ligature may be tied onto the newly placed attachment and drawn in the direction of the target site in the dental arch.
During exposure of the crown of a tooth, instrumentation of the enamel surface will hamper neither the eruption process nor the quality of the treated result. On the other hand, exposure and instrumentation of the root surface are potentially damaging. Exposing root surface presupposes that the natural attachment of the tooth at the CEJ will have been ruptured and, in consequence, renewed attachment will probably only be able to be established more apically. Indeed, there are yet more undesirable results of exposing root surface: periodontal fibres are severed and cementum exposed and subjected to drying (from the suction and air syringe) and contact with foreign substances (etchant, bonding materials). This can in due course lead to the initiation of a resorption process on the root surface, as well as to ankylosis and to total failure of eruption, as we shall read in Chapter 10. Even more common possible consequences include seriously reduced bone support, long clinical crowns and poor gingival attachment and quality.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Orthodontic Treatment of Impacted Teeth»
Представляем Вашему вниманию похожие книги на «Orthodontic Treatment of Impacted Teeth» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.


Обсуждение, отзывы о книге «Orthodontic Treatment of Impacted Teeth» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.