Adrian Becker - Orthodontic Treatment of Impacted Teeth
Здесь есть возможность читать онлайн «Adrian Becker - Orthodontic Treatment of Impacted Teeth» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Orthodontic Treatment of Impacted Teeth
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Orthodontic Treatment of Impacted Teeth: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Orthodontic Treatment of Impacted Teeth»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Provides protocols for common cases as well as complex and rare presentations Contains individual chapters on the specific aspects of the diagnosis and treatment of impaction in each of the different types of teeth Covers prevalence, etiology, diagnosis, attitudes to treatment, treatment timing, treatment methods, and prognosis Features more than 1,000 high-quality color images and illustrations
remains essential reading for all specialist orthodontists, academic researchers and instructors, oral and maxillofacial surgeons, and advanced students in orthodontics.
Orthodontic Treatment of Impacted Teeth — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Orthodontic Treatment of Impacted Teeth», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
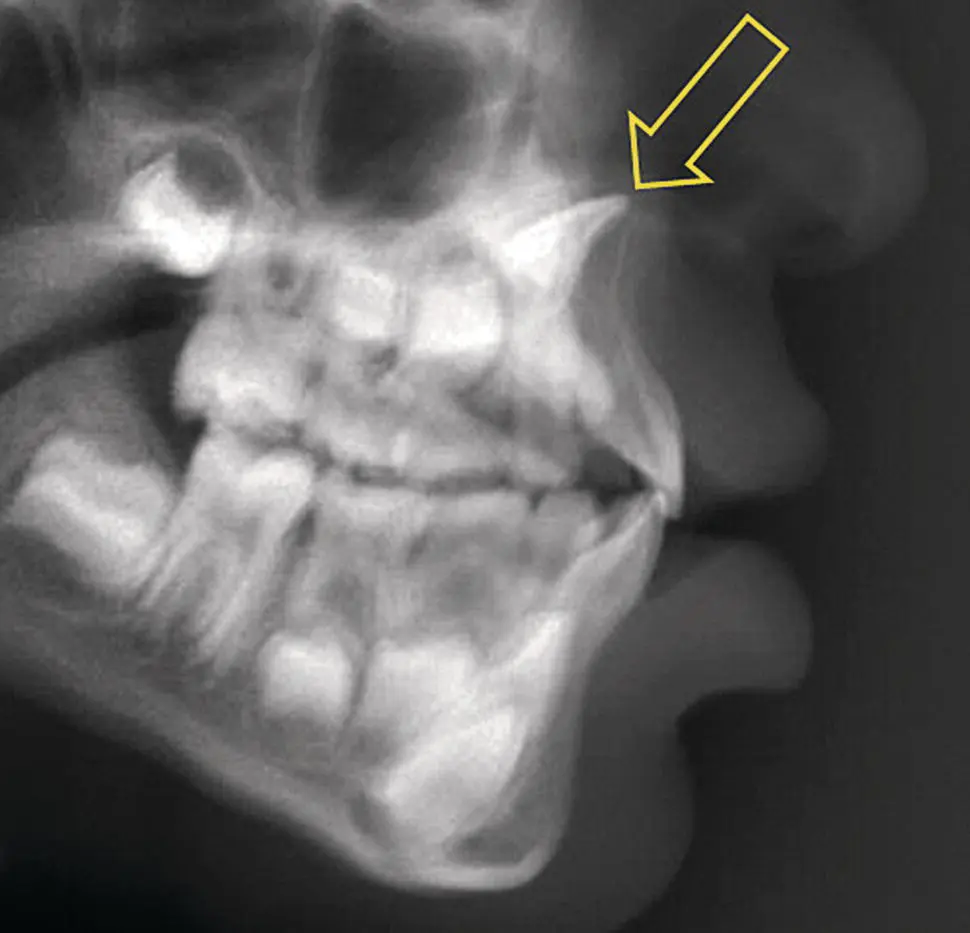
Fig. 4.12 A dilacerated central incisor (arrow) seen in a lateral cephalometric radiograph.
For maxillary canines, the lateral view is extremely useful. It should be remembered that most impacted maxillary canines are diagnosed in the full permanent dentition, when all the other teeth have erupted. This permits clear radiographic imaging of the canine when it is sited at a higher level than the other teeth.
A postero‐anterior cephalometric radiograph is used less routinely in orthodontics, but it does offer the clinician the opportunity to view the maxilla in a different plane, the true postero‐anterior view ( Figure 4.10b), which is at right angles to the lateral cephalogram. The overlap of structures of the base of the skull and the maxilla renders detail of individual teeth less clear, but a good postero‐anterior radiograph will show the height of both the crown and the root of a significantly displaced tooth, as with the lateral radiograph. This view also shows whether the root apex of an ectopic posterior tooth is in the line of the arch and how far the crown is deflected in the palatal direction. The bucco‐lingual tilt of the long axis of the tooth will be plainly visible ( Figure 4.10b). However, the view is less practical in the mandible, where the left and right sides of its V‐shaped body converge, as they proceed forward towards the anterior midline and are thus oblique to the central ray. There is usually excessive overlap, more radio‐opaque bone and difficulty in discerning even markedly bucco‐lingually displaced teeth. For structures close to the midline, the panoramic view offers a very similar representation ( Figure 4.10c) and a much clearer picture. Since this view is a rotational tomograph, it eliminates all structures that are either lingually or buccally outside the narrow focal trough at which it is aimed.
An occlusal projection of the anterior maxilla ( Figure 4.2) offers the possibility of viewing in the third plane of space, at right angles to each of the two earlier radiographs, and recording the position of the displaced incisor or canine without overlap. However, for maximum effect it is important to project the X‐ray beam through the long axis of the maxillary teeth, as we have just described.
Any two of these three views (the lateral cephalogram or tangential view, the postero‐anterior cephalogram view and the true occlusal view) will provide complete information regarding every aspect of the height, bucco‐lingual and mesio‐distal location of the crown and the root, and the degree of tilt of the long axis of the impacted tooth and its relation to neighbouring teeth. The postero‐anterior cephalogram and the occlusal views, however, are not always as clear as is desirable, and they may need to be repeated or discarded. In a case of bilateral canine impaction, the lateral cephalometric or the tangential view may create confusion, since one canine will be superimposed on the other and distinguishing them may be a problem, whereas other views will usually facilitate differentiation. Two identically oriented and superimposed canines ( Figure 4.10) will obviously not need to be differentiated.
It is essential to be aware that many of the radiographs that we take for other reasons should always be scrutinized for useful information regarding positions of unerupted teeth. This is particularly so regarding cephalograms, whose principal aim is to measure and compare angles and distances on tracings of specific landmarks on the radiograph. Sadly, these potentially valuable views are often filed away without sufficient thought.
From these projections, it is very easy to build up a 3D picture of the exact position and angulation of the impacted tooth and to define the type of movement that will be necessary to bring the tooth into alignment. When a composite mental reconstruction is made of the position of the unerupted tooth in space, the design of the appliance needed to resolve the impaction is simplified and fewer surprises are likely to be encountered. It is, however, a sine qua non in all these cases to examine a periapical view of the tooth in order to eliminate the possibility of local pathology, which is much more likely to be missed on the extra‐oral views.
The foregoing description has covered the various methods available for envisioning the anatomical form and 3D location of unerupted teeth, using plain film radiography. We have seen that, in order to achieve an adequate picture of the relationships between the crowns of these teeth and the surrounding anatomical structures, including adjacent teeth, information gleaned from several different types of view needs to be put together to make up the complex picture. Nevertheless, even when enough information is available, mistakes and misdiagnoses are sometimes made by experienced orthodontists [6], occasionally with serious repercussions for the patient.
It would be appropriate now to consider the question of whether the same degree of precision in root apex location and 3D root orientation is essential for both the orthodontist and the surgeon. From the point of view of the oral surgeon, diagnosis of the position of the crown, buccal or palatal to the line of the arch, is generally all that is needed, regardless of whether the tooth is to be exposed for orthodontic alignment or extracted. The position of the root apex and the orientation of the long axis of the tooth are irrelevant for surgical exposure. If the tooth is to be extracted in one piece, careful dissection of the tissue surrounding the crown and dislodging it with an elevator or extraction forceps will deliver the tooth, together with its root. Even if the root portion is sectioned and scheduled for extraction, after removal of the crown portion, its general orientation and apex position can be determined by the anatomy and general orientation of the crown. For these reasons and until CBCT became first choice, many surgeons have had to rely solely on the tube shift parallax method of positional diagnosis for exposure or extraction of impacted teeth, and have done so with a degree of exaggerated confidence. However, today the majority will overwhelmingly prefer cross‐sectional slices reconstructed from a CBCT series.
From the point of view of the orthodontist, however, while the position of the crown is important, the position of the apex and the orientation of the long axis of the tooth are crucial. When the root apex of the impacted tooth is displaced, re‐siting it in its correct position is fraught with technical difficulty and can only be done once the crown has been brought into its place in the arch and ligated into the main archwire. As we shall discuss in Chapter 7, root movement is the most damaging movement to the root itself and to the supporting tissues. It has been shown to be one of the factors that most undermine the periodontal prognosis of the treated result [14–16]. Orthodontists cannot be expected to be confident in their ability to bring a tooth into full alignment if an accurate 3D diagnosis of its position is not available. In the event, a surgical exposure may be attempted from the wrong side of the alveolus and unnecessary damage will ensue. Alternatively, the impacted tooth may be drawn in the wrong direction and will be brought into contact with the root of an adjacent tooth, which may lead to resorption of that root or to the blocking of further progress. The reader is referred to Chapter 18for an illustrated description of failures and how most of these were due to positional misdiagnosis.
Unfortunately, the above‐mentioned plane radiograph methods exhibit many shortcomings. This is particularly true in relation to the bucco‐lingual plane. Undoubtedly, the most difficult aspect to define is the relative proximity of the impacted tooth to the root of an adjacent tooth on which its image is superimposed in the bucco‐lingual plane, as seen on a periapical, anterior occlusal, panoramic or cephalometric radiographs. Whether there is a small distance between them or whether the crown of the impacted tooth lies in a resorption crater on the palatal or labial aspect of the root of an incisor may be impossible to determine using plane 2D radiography. As a result, an undiagnosed and severely resorbed tooth, with a poor long‐term prognosis, may be mistakenly included as an integral but ‘weak link’ in the final scheme of the dentition in a projected treatment plan [17].
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Orthodontic Treatment of Impacted Teeth»
Представляем Вашему вниманию похожие книги на «Orthodontic Treatment of Impacted Teeth» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.


Обсуждение, отзывы о книге «Orthodontic Treatment of Impacted Teeth» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.