Adrian Becker - Orthodontic Treatment of Impacted Teeth
Здесь есть возможность читать онлайн «Adrian Becker - Orthodontic Treatment of Impacted Teeth» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Orthodontic Treatment of Impacted Teeth
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Orthodontic Treatment of Impacted Teeth: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Orthodontic Treatment of Impacted Teeth»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Provides protocols for common cases as well as complex and rare presentations Contains individual chapters on the specific aspects of the diagnosis and treatment of impaction in each of the different types of teeth Covers prevalence, etiology, diagnosis, attitudes to treatment, treatment timing, treatment methods, and prognosis Features more than 1,000 high-quality color images and illustrations
remains essential reading for all specialist orthodontists, academic researchers and instructors, oral and maxillofacial surgeons, and advanced students in orthodontics.
Orthodontic Treatment of Impacted Teeth — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Orthodontic Treatment of Impacted Teeth», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
This, however, is an overly simplistic diagnosis, since indeed there are two possible conclusions to the practitioner’s observations. It is of paramount importance to carefully study the radiographs in order to distinguish between these two possibilities and thereby avoid unnecessary harm being inflicted on the child and the parents.
The initial conclusion to which the practitioner came would indeed be correct if the radiographs were to show that the unerupted permanent canines and premolars had completed most of their expected root length, showing that the child’s dental age corresponded with his chronological age. In the present case ( Figure 1.1), the deciduous teeth had not shed naturally, presumably due to insufficient resorption of their roots constituting an impediment to the normal eruption of the permanent teeth. Their permanent successors must then strictly be defined as having delayed eruption. The logical line of treatment would be to extract the deciduous teeth on the grounds that their continued presence defines them as over‐retained.
However, there is a second possibility, where the radiographs reveal relatively little root development, more closely corresponding on the tooth development chart ( Figure 1.2) to the picture of a 9‐year‐old child. The child’s birth certificate has indicated the age of 12 years and this may well be corroborated by body size and development and even by intelligence level. Nevertheless, her dentition is that of a child three years younger, thus determining dental age as 9 years. Extraction of deciduous teeth in these circumstances would be the wrong line of treatment, since it is to be expected that these teeth will shed normally at the appropriate dental age. Early extraction may lead to the undesired characteristic consequences of early extraction, performed for a completely different reason.
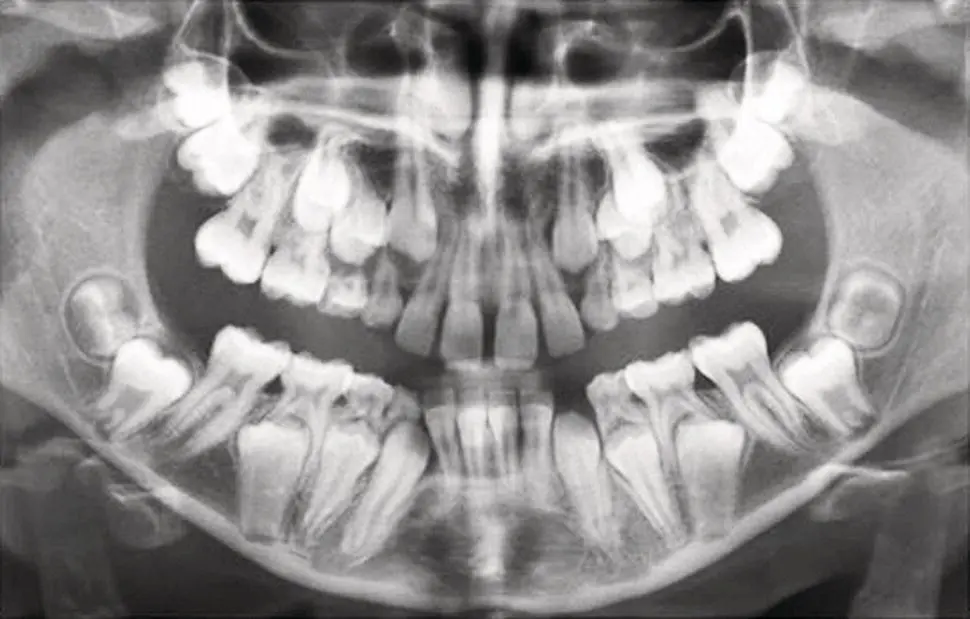
Fig. 1.1 The advanced root development of the canines and premolars indicates a dental age of 12–13 years, despite the presence of 11 deciduous teeth in this 10‐year‐old child. This defines the deciduous teeth as over‐retained and extraction is their appropriate treatment. A note should be made and follow‐up is needed regarding the relatively slow eruptive progress of the second permanent molars.
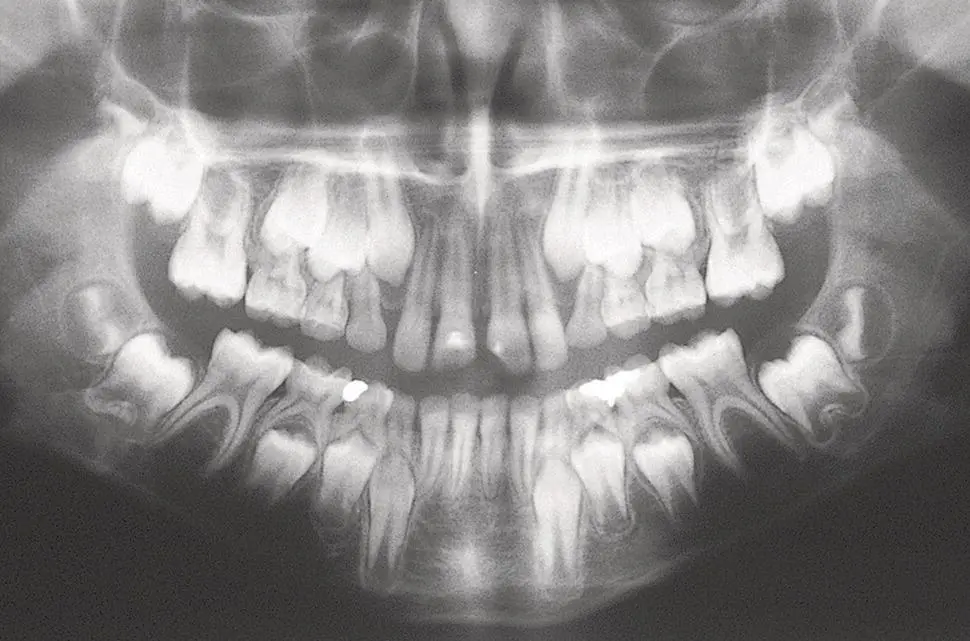
Fig. 1.2 A 12‐year‐old patient with root development indicating the late dental age of 9 years. Extraction of deciduous teeth is contraindicated
An additional parameter of teeth development must also be considered. Although on average, central incisors, canines and first and second molars in the maxilla show identical rates of development of one side of the mouth compared to the other, this may not be true for certain specific teeth. There may be a marked variation between right and left sides in the development rate of maxillary lateral incisors and mandibular second premolars and, less commonly, of maxillary second premolars.
In the same way that we may determine the patient’s overall dental age, these identical principles also serve to enable us to diagnose the dental age of the patient’s individual unerupted permanent teeth. However, because developmental variation is found within these different groups of teeth, the developmental stage of a single tooth cannot be used as an indicator for overall dental development and dental age must be evaluated employing a comprehensive, all‐round assessment. Only then can a definitive determination be offered.
Accurate assessment of dental age is critical in deciding when to treat a patient in general and in regard to the treatment of impacted teeth in particular.
We are now in a position to define the terms that we shall use throughout this text, as follows:
Retained deciduous tooth: This term has a positive connotation and refers to a tooth that remains in place beyond its normal, chronological shedding time due to the absence, or retarded development, of the permanent successor. A radiograph of the permanent successor is required in order to determine the presence and developmental status of the unerupted permanent tooth.
Over‐retained deciduous tooth: In contrast, this term has a negative connotation and refers to a tooth whose unerupted permanent successor exhibits root development in excess of two‐thirds of its expected final length ( Figure 1.3). Here too, a radiograph of the permanent successor is required in order to determine the status of the deciduous tooth and its implied treatment. Fig. 1.3 The mandibular left second deciduous molar is retained (extraction contraindicated), since the root development of its successor is inadequate for normal eruption. The right maxillary deciduous canine, in contrast, is over‐retained (extraction advised), since the long root of its successor illustrates delayed eruption.
Permanent tooth with delayed eruption: This term refers to an unerupted tooth whose root is developed in excess of two‐thirds of its expected final length and whose spontaneous eruption may nevertheless be expected within a reasonable time.
Impacted tooth: This refers to a tooth whose root is developed in excess of two‐thirds of its expected final length, but which is not expected to erupt in a reasonable time.
When assessing the dental age of the patient, it is important to emphasize that one should not include the maxillary lateral incisors, the mandibular second premolars and the third molars in this calculation. The development timetable of these teeth is not always in line with that of the patient’s other, ontologically more stable teeth [9, 10]. These are the same teeth that are most frequently congenitally missing in cases of partial anodontia (hypodontia) or oligodontia. Indeed, reduced size, poorly contoured crown form and late development of these teeth are all considered microforms of congenital absence [9–12]. The variation in their timing is, however, always expressed as lateness and they are never seen in a chronologically more advanced state of development than the other teeth. If the individual dental age of any of these variable groups of teeth is advanced, then so too is the dental age of the entire dentition in which they are to be found.
In summary, therefore, we may assert as follows:
All orthodontists must have at their fingertips the ages at which the permanent teeth normally erupt.
Permanent teeth normally erupt when approximately two‐thirds of their final root length has developed.
The remainder of the root reaches apexification approximately 2½–3 years after eruption.
Determining the closed apex of the tooth on a radiograph is usually an easy and accurate parameter to establish.
Determining the completed proportion of the root of a tooth, whose final completed length is unknown, is not an assessment that can be performed accurately. It rather falls into the realm of informed guesswork.
Having now set out the principles upon which dental age may be assessed, we must turn to the practical side of translating these principles into clinical terms in a logical, systematic and didactic manner. The simplistic way of adopting the above principles would be to take the panoramic radiograph or full‐mouth periapical survey and then work around each dental arch from one tooth to the next, individually and from left to right, upper to lower, evaluating each tooth in turn. This would then require coordinating all the individual results and computing a final figure that is the dental age of the patient. The resulting conclusion would have to be compared against the values seen on an idealized chart of the norms for a given population [1, 4, 13]. Although this method delivers accuracy, it requires a considerable time and it is likely to take an hour or so to reach the final conclusion. It is an arduous and tedious endeavour, which does not lend itself to the conditions that are present in a busy clinical orthodontic practice.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Orthodontic Treatment of Impacted Teeth»
Представляем Вашему вниманию похожие книги на «Orthodontic Treatment of Impacted Teeth» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.


Обсуждение, отзывы о книге «Orthodontic Treatment of Impacted Teeth» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.