Michael J. Neal - Medical Pharmacology at a Glance
Здесь есть возможность читать онлайн «Michael J. Neal - Medical Pharmacology at a Glance» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Medical Pharmacology at a Glance
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Medical Pharmacology at a Glance: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Medical Pharmacology at a Glance»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
is the ideal companion for all medical and healthcare students, providing a visual overview of pharmacology, and describing the basic principles of drug action, interaction, absorption, and excretion. Clear and accessible chapters organised around common diseases and conditions facilitate efficient clinical learning, and include references to drug classes and side effects, disease pathophysiology, prescribing guidelines, and more.
Now in its ninth edition, this leading guide has been thoroughly updated to reflect current guidelines and drug information. This edition features new and revised illustrations, additional pedagogical tools, and enhanced online content. Widely recognised as both the best introduction to medical pharmacology and the perfect revision tool for USMLE and pharmacology exams, this invaluable guide:
Covers a wide range of drugs used to treat conditions such as hypertension, anaemias, cancer, and affective disorders Explains drug mechanisms and the principles of drug action Discusses practical topics including drug misuse, drug indications, and side effects Includes a companion website featuring online cases, flashcards, and a list of core drugs
Medical Pharmacology at a Glance — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Medical Pharmacology at a Glance», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Nicotinic effectsinclude stimulation of all autonomic ganglia. However, the action of acetylcholine on ganglia is relatively weak compared with its effect on muscarinic receptors, and so parasympathetic effects predominate. The nicotinic actions of acetylcholine on the sympathetic system can be demonstrated, for example, on cat blood pressure, by blocking its muscarinic actions with atropine. High intravenous doses of acetylcholine then cause a rise in blood pressure, because stimulation of the sympathetic ganglia and adrenal medulla now results in vasoconstriction and tachycardia.
8 Autonomic drugs acting at cholinergic synapses
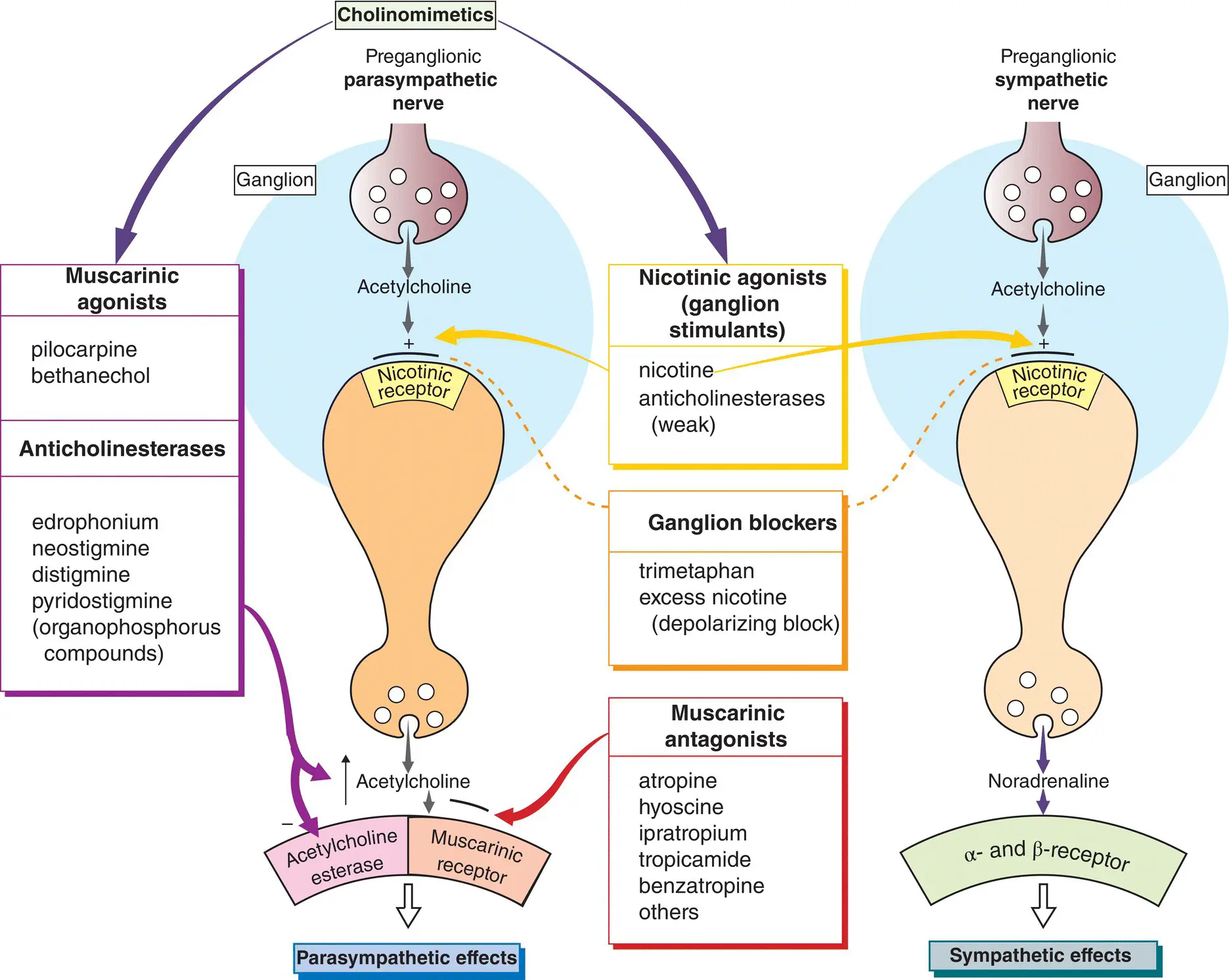
Acetylcholine released from the terminals of postganglionic parasympathetic nerves (left,  ) produces its actions on various effector organs by activating muscarinic receptors(
) produces its actions on various effector organs by activating muscarinic receptors(  ). The effects of acetylcholine are usually excitatory, but an important exception is the heart, which receives inhibitory cholinergic fibres from the vagus ( Chapter 17). Drugs that mimic the effects of acetylcholine are called cholinomimeticsand can be divided into two groups:
). The effects of acetylcholine are usually excitatory, but an important exception is the heart, which receives inhibitory cholinergic fibres from the vagus ( Chapter 17). Drugs that mimic the effects of acetylcholine are called cholinomimeticsand can be divided into two groups:
drugs that act directly on receptors (nicotinic and muscarinic agonists); and
anticholinesterases, which inhibit acetylcholinesterase and so act indirectly by allowing acetylcholine to accumulate in the synapse and produce its effects.
Muscarinic agonists(top left) have few uses, but pilocarpine(as eyedrops) is sometimes used to reduce intraocular pressure in patients with glaucoma ( Chapter 10). Bethanecholwas used to stimulate the bladder in urinary retention, but it has been superseded by catheterization.
Anticholinesterases(bottom left) have relatively little effect at ganglia and are used mainly for their nicotinic effects on the neuromuscular junction. They are used in the treatment of myasthenia gravis and to reverse the effects of competitive muscle relaxants used during surgery ( Chapter 6).
Muscarinic antagonists(bottom middle) block the effects of acetylcholine released from postganglionic parasympathetic nerve terminals. Their effects can, in general, be worked out by examination of the figure in Chapter 7. However, parasympathetic effector organs vary in their sensitivity to the blocking effect of antagonists. Secretions of the salivary, bronchial and sweat glands are most sensitive to blockade. Higher doses of antagonist dilate the pupils, paralyze accommodation and produce tachycardia by blocking vagal tone in the heart. Still higher doses inhibit parasympathetic control of the gastrointestinal tract and bladder. Gastric acid secretion is most resistant to blockade ( Chapter 12).
Atropine, hyoscine(scopolamine) or other antagonists are used:
1 in anaesthesia to block vagal slowing of the heart and to inhibit bronchial secretion;
2 to reduce intestinal spasm in, for example, irritable bowel syndrome ( Chapter 13);
3 in Parkinson’s disease (e.g. benzatropine, Chapter 26);
4 to prevent motion sickness (hyoscine, Chapter 30);
5 to dilate the pupil for ophthalmological examination (e.g. tropicamide) or to paralyse the ciliary muscle ( Chapter 10);
6 as a bronchodilator in asthma (ipratropium, Chapter 11) and
7 in urinary incontinence antimuscarinic drugs e.g. solfenacin, darifenacin reduce detrusor muscle overactivity.
Transmission at autonomic ganglia (  ) can be stimulated by nicotinic agonists (top middle) or blocked by drugs that act specifically on the ganglionic neurone nicotinic receptor/ionophore (middle). Nicotinic agonists are of no clinical use and ganglion blocking drugs, e.g. hexamethonium, are only of historical interest.
) can be stimulated by nicotinic agonists (top middle) or blocked by drugs that act specifically on the ganglionic neurone nicotinic receptor/ionophore (middle). Nicotinic agonists are of no clinical use and ganglion blocking drugs, e.g. hexamethonium, are only of historical interest.
Cholinergic nerve terminalsin the autonomic nervous system synthesize, store and release acetylcholine in essentially the same way as at the neuromuscular junction ( Chapter 6). Acetylcholinesterase is bound to both the pre‐ and postsynaptic membranes.
Cholinomimetics
Muscarinic agonists
These directly activate muscarinic receptors, usually producing excitatory effects. An important exception is the heart, where activation of the predominantly M 2‐receptors has inhibitory effects on the rate and force of (atrial) contraction. The M 2‐receptors are negatively coupled by a G‐protein (G 1) to adenylyl cyclase, which explains the negative inotropic effect of acetylcholine. Subunits (βγ)) of G 1directly increase K +conductances in the heart causing hyperpolarization and bradycardia ( Chapter 17). Acetylcholine stimulates glandular secretion and causes contraction of smooth muscle by activating M 3‐receptors, which are coupled to the formation of inositol‐1,4,5‐trisphosphate (InsP 3) and diacylglycerol ( Chapter 1). InsP 3increases cytosolic Ca 2+, thus triggering muscle contraction or glandular secretion. An intravenous injection of acetylcholine causes vasodilatation indirectly by releasing nitric oxide (NO) from vascular endothelial cells ( Chapter 16). However, most blood vessels have no parasympathetic innervation and so the physiological function of vascular muscarinic receptors is uncertain.
Choline esters
Bethanecholis a quaternary compound that does not penetrate the blood–brain barrier. Its actions are much more prolonged than those of acetylcholine, because it is not hydrolyzed by cholinesterase.
Pilocarpinepossesses a tertiary N atom, which confers increased lipid solubility. This enables the drug to penetrate the cornea readily when applied locally, and enter the brain when given systemically.
Anticholinesterases
These are indirectly acting cholinomimetics. The commonly used anticholinesterase drugs are quaternary compounds that do not pass the blood–brain barrier and have negligible central effects. They are poorly absorbed orally. Physostigmine(eserine) is much more lipid soluble. It is well absorbed after oral or local administration (e.g. as eyedrops) and passes into the brain.
Mechanism of action
Initially, acetylcholine binds to the active site of the esterase and is hydrolyzed, producing free choline and acetylated enzyme. In a second step, the covalent acetyl–enzyme bond is split with the addition of water. Edrophoniumis the main example of a reversible anticholinesterase. It binds by electrostatic forces to the active site of the enzyme. It does not form covalent bonds with the enzyme and so is very short acting (2–10 min). The carbamate esters (e.g. neostigmine, pyridostigmine) undergo the same two‐step process as acetylcholine, except that the breakdown of the carbamylated enzyme is much slower (30 min to 6 h). Organophosphorus agents result in a phosphorylated enzyme active site. The covalent phosphorus–enzyme bond is very stable and the enzyme is inactivated for hundreds of hours. For this reason, the organophosphorus compounds are referred to as irreversible anticholinesterases. They are extremely toxic and are used as insecticides (parathion, malathion) and chemical warfare agents (e.g. sarin). Malathion is used topically in the treatment of scabies and head lice.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Medical Pharmacology at a Glance»
Представляем Вашему вниманию похожие книги на «Medical Pharmacology at a Glance» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.





Обсуждение, отзывы о книге «Medical Pharmacology at a Glance» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.