Michael J. Neal - Medical Pharmacology at a Glance
Здесь есть возможность читать онлайн «Michael J. Neal - Medical Pharmacology at a Glance» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Medical Pharmacology at a Glance
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Medical Pharmacology at a Glance: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Medical Pharmacology at a Glance»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
is the ideal companion for all medical and healthcare students, providing a visual overview of pharmacology, and describing the basic principles of drug action, interaction, absorption, and excretion. Clear and accessible chapters organised around common diseases and conditions facilitate efficient clinical learning, and include references to drug classes and side effects, disease pathophysiology, prescribing guidelines, and more.
Now in its ninth edition, this leading guide has been thoroughly updated to reflect current guidelines and drug information. This edition features new and revised illustrations, additional pedagogical tools, and enhanced online content. Widely recognised as both the best introduction to medical pharmacology and the perfect revision tool for USMLE and pharmacology exams, this invaluable guide:
Covers a wide range of drugs used to treat conditions such as hypertension, anaemias, cancer, and affective disorders Explains drug mechanisms and the principles of drug action Discusses practical topics including drug misuse, drug indications, and side effects Includes a companion website featuring online cases, flashcards, and a list of core drugs
Medical Pharmacology at a Glance — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Medical Pharmacology at a Glance», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
ACh receptor
This can be activated by nicotine and, for this reason, is called a nicotinic receptor. * The receptor–channel complex is pentameric and is constructed from four different protein subunits (ααβγε in the adult) that span the membrane and are arranged to form a central pore (channel) through which cations (mainly Na +) flow. ACh molecules bind to the two α‐subunits, inducing a conformational change that opens the channel for about 1 ms.
Myasthenia gravis
Myasthenia gravis is an autoimmune disease in which neuromuscular transmission is defective. Circulating heterogeneous immunoglobulin G (IgG) antibodies cause a loss of functional ACh receptors in skeletal muscle. Symptomatic relief to counter the loss of receptors is obtained by the use of an anticholinesterase, usually pyridostigmine. Immunological treatment includes the administration of prednisoloneor azathioprine( Chapter 45). Plasmapheresis, in which blood is removed and the cells returned, may improve motor function, presumably by reducing the level of immune complexes. Thymectomy may be curative.
Presynaptic agents
Drugs inhibiting ACh release
Botulinum toxin is produced by Clostridium botulinum (an anaerobic bacillus, see Chapter 37). The exotoxin is extraordinarily potent and prevents ACh release by enzymatically cleaving the proteins (e.g. synaptobrevin) required for docking of vesicles within the presynaptic membrane. C. botulinum is very rarely responsible for serious food poisoning in which the victims exhibit progressive parasympathetic and motor paralysis. Botulinum toxin type Ais used in the treatment of certain dystonias, such as blepharospasm (spasmodic eye closure), hemifacial spasm and spasmodic torticollis. In these conditions, low doses of toxin are injected into the appropriate muscle to produce paralysis that persists for about 12 weeks. Botulinum toxin is used to treat urinary incontinence in patients with spinal cord injury in patients with MS. Injected directly into the bladder, the toxin increases storage capacity and decreases incontinence.
Competitive neuromuscular blocking drugs
In general, the competitive neuromuscular blocking drugs are bulky, rigid molecules and most have two quaternary N atoms. Neuromuscular blocking drugs are given by intravenous injection and are distributed in the extracellular fluid. They do not pass the blood–brain barrier or the placenta. The choice of a particular drug is often determined by the side‐effects produced. These include histamine release, vagal blockade, ganglion blockade and sympathomimetic actions. The onset of action and the duration of action of neuromuscular blocking drugs depend on the dose, but also on other factors (e.g. prior use of suxamethonium, anaesthetic agent used).
Pancuroniumis an aminosteroid neuromuscular blocking drug with a relatively long duration of action. It does not block ganglia or cause histamine release. However, it has a dose‐related atropine‐like effect on the heart that can produce tachycardia.
Vecuronium and atracuriumare commonly used agents. Vecuroniumhas no cardiovascular effects. It depends on hepatic inactivation and recovery can occur within 20–30 min, making it an attractive drug for short procedures. Atracuriumhas a duration of action of 15–30 min. It is only stable when kept cold and at low pH. At body pH and temperature, it decomposes spontaneously in plasma and therefore does not depend on renal or hepatic function for its elimination. It is the drug of choice in patients with severe renal or hepatic disease. Atracurium may cause histamine release with flushing and hypotension. Cisatracuriumis an isomer of atracurium. Its main advantage is that it does not cause histamine release and its associated cardiovascular effects.
Rocuroniumhas an intermediate duration of action of about 30 min, but with a rapid onset of action (1–2 min) comparable with that of suxamethonium (1–1.5 min). It has minimal cardiovascular effects.
Reversal of neuromuscular blockadeNeostigmine IV quickly reverses the action of competitive neuromuscular blockers. Atropine or glycopyrronium is given first to prevent parasympathetic effects. Sugammadexbinds to the steroidal drugs vecuronium and rocuronium forming an inactive complex.
Depolarizing neuromuscular blocking drugs
Suxamethonium(succinylcholine) is used because of its rapid onset and very short duration of action (2–6 min). The drug is normally hydrolysed rapidly by plasma pseudocholinesterase, but a few people (about 1 in 3000) inherit an atypical form of the enzyme and, in such individuals, the neuromuscular block may last for hours. Suxamethonium depolarizes the endplate and, because the drug does not dissociate rapidly from the receptors, a prolonged receptor activation is produced. The resulting endplate depolarization initially causes a brief train of muscle action potentials and muscle fibre twitches. Neuromuscular block then occurs as a result of several factors which include: (i) inactivation of the voltage‐sensitive Na +channels in the surrounding muscle fibre membrane, so that action potentials are no longer generated; and (ii) transformation of the activated receptors to a ‘desensitized’ state, unresponsive to ACh. The main disadvantage of suxamethonium is that the initial asynchronous muscle fibre twitches cause damage, which often results in muscle pains the next day. The damage also causes potassium release. Repeated doses of suxamethonium may cause bradycardia in the absence of atropine (a muscarinic effect).
Note
1 *Pentameric nicotinic receptors also occur in autonomic ganglia and the brain. They have variants of the α‐ and β‐subunit and a different pharmacology.
7 Autonomic nervous system
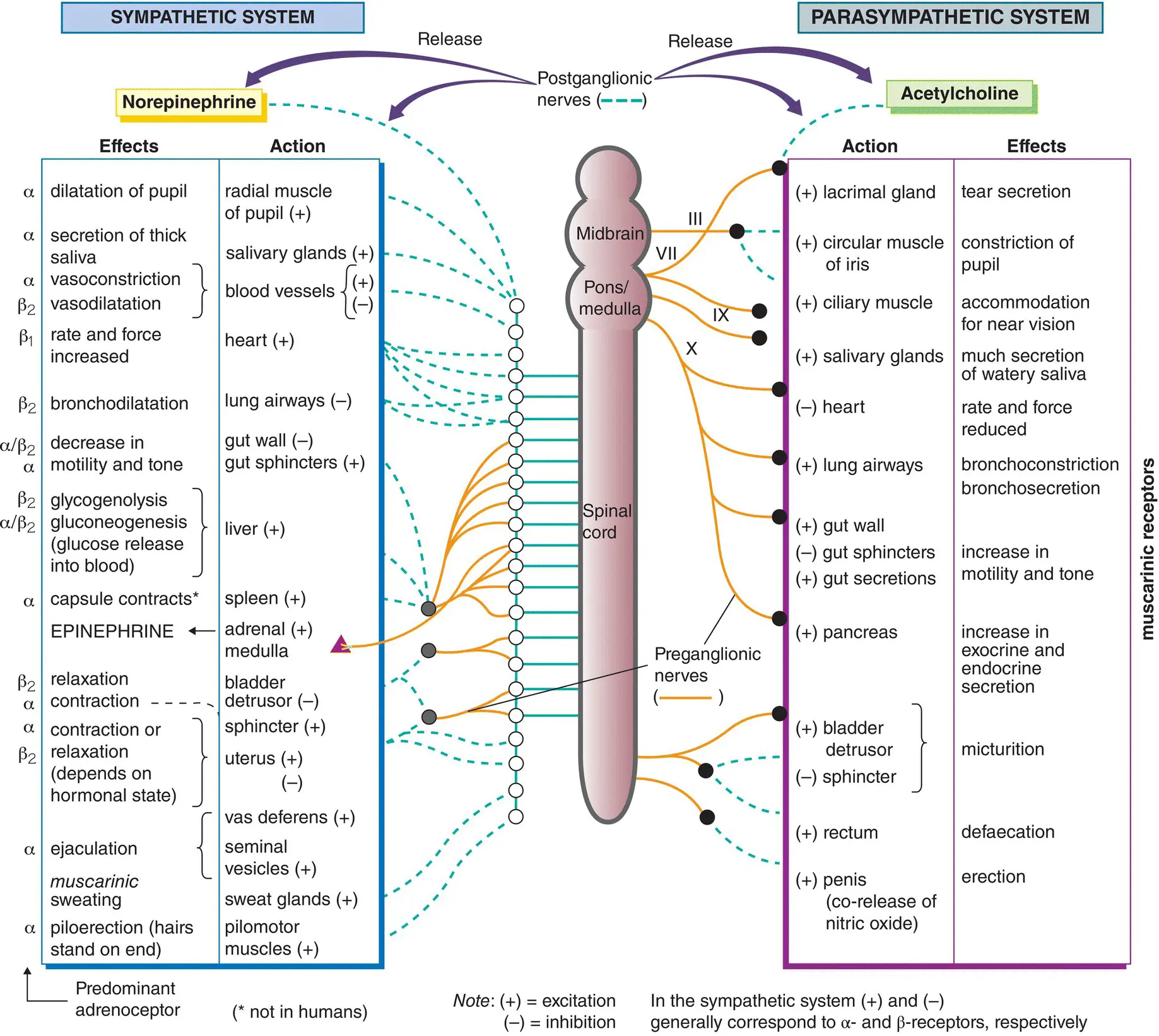
Many systems of the body (e.g. digestion, circulation) are controlled automatically by the autonomic nervous system (and the endocrine system). Control of the autonomic nervous system often involves negative feedback, and there are many afferent (sensory) fibres that carry information to centres in the hypothalamus and medulla. These centres control the outflow of the autonomic nervous system, which is divided on anatomical grounds into two major parts: the sympathetic system(left) and the parasympathetic system(right). Many organs are innervated by both systems, which in general have opposing actions. The actions of sympathetic (left) and parasympathetic (right) stimulation on different tissues are indicated in the inner columns, and the resulting effects on different organs are shown in the outer columns.
The sympathetic nerves (left, ) leave the thoracolumbar region of the spinal cord (T1–L3) and synapse either in the paravertebral ganglia(  ) or in the prevertebral ganglia(
) or in the prevertebral ganglia(  ) and plexuses in the abdominal cavity. Postganglionic non‐myelinated nerve fibres (left,
) and plexuses in the abdominal cavity. Postganglionic non‐myelinated nerve fibres (left,  ) arising from neurones in the ganglia innervate most organs of the body (left).
) arising from neurones in the ganglia innervate most organs of the body (left).
Интервал:
Закладка:
Похожие книги на «Medical Pharmacology at a Glance»
Представляем Вашему вниманию похожие книги на «Medical Pharmacology at a Glance» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.





Обсуждение, отзывы о книге «Medical Pharmacology at a Glance» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.