Autoimmune Liver Disease
Здесь есть возможность читать онлайн «Autoimmune Liver Disease» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Autoimmune Liver Disease
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Autoimmune Liver Disease: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Autoimmune Liver Disease»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
, practitioners will learn about the current state of autoimmune liver disease and how to focus on their diagnosis and treatment. The four-part book begins with a thorough investigation of current immunological thinking as it relates to the autoimmunity of the liver. It also covers the four major hepatic autoimmune liver diseases in both adults and children, their management and the role of liver transplantation, and learned approaches to patient management and empowerment.
Expert authors in the field have come together to provide a thorough examination of autoimmune liver disease to help support clinicians assisting patients. The text provides an in-depth look at topics including:
● The four major hepatic autoimmune liver diseases, their diagnosis, and potential disease management
● The use (and misuse) of autoantibodies in diagnosis and treatment
● The role and timing of liver transplantation and the impact of recurrent autoimmune liver disease as well as de novo autoimmune hepatitis
● Optimal approaches to managing patients and keeping care personalised
With breadth, depth and current-day relevance,
sheds light on recent developments in management of liver disease for practitioners, nurses, and health care professionals.
Autoimmune Liver Disease — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Autoimmune Liver Disease», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
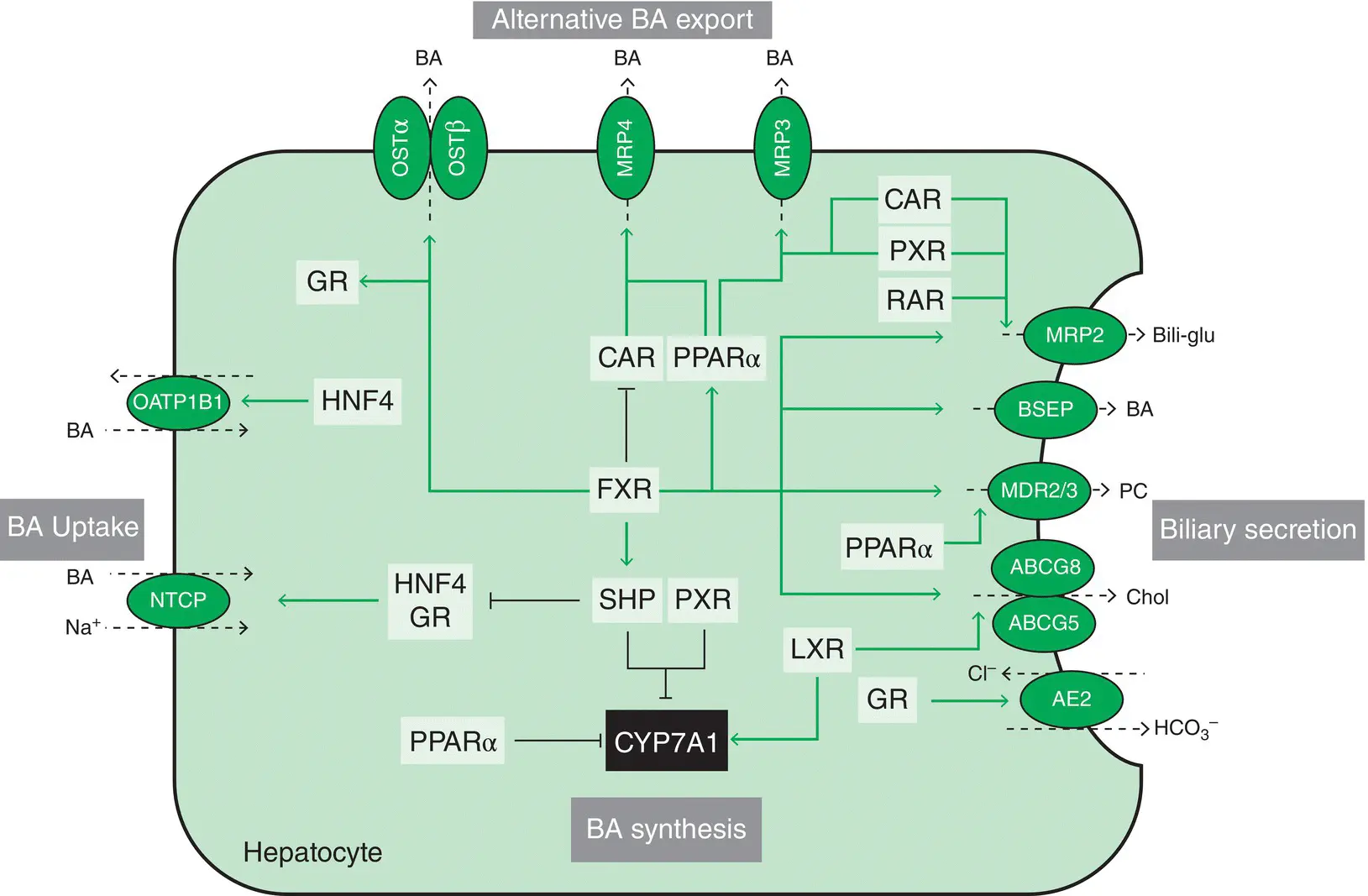
Figure 1.1 Transcriptional regulation of hepatocellular bile formation. Expression of hepatobiliary transporters in hepatocytes determines hepatic bile acid (BA) flux and hepatocellular concentrations of these potentially toxic metabolites. To ensure the balance between synthesis, uptake and excretion, expression of hepatobiliary transporters is tightly regulated by nuclear receptors (NRs). NRs provide a network of negative feedback and positive feed‐forward mechanisms for the control of intracellular concentration of biliary constituents, which are often also ligands for these NRs. BA‐activated FXR is a central player in this network, that represses hepatic BA uptake (NTCP) and (via SHP) synthesis (CYP7A1), promotes bile secretion via induction of canalicular transporters (BSEP, MRP2, ABCG5/8, MDR3), and induces BA elimination via alternative export systems at the hepatic basolateral (sinusoidal) membrane (OSTα/β). Several NR pathways converge at the level of CYP7A1 as the rate‐limiting enzyme in BA synthesis. CAR and PXR facilitate adaptation to increased intracellular BA concentrations by upregulation of alternative hepatic export routes (MRP3 and MRP4) and induction of detoxification enzymes (not shown). Together with RAR, these xenobiotic receptors also regulate the canalicular expression of MRP2. Cholesterol sensor LXR promotes biliary cholesterol excretion via ABCG5/8. Stimulation of AE2 expression by GR stimulates biliary bicarbonate secretion thus reducing bile toxicity. Green arrows indicate stimulatory and red lines suppressive effects on target genes. Bili‐glu, bilirubin glucuronide; BSEP, bile salt export pump; CAR, constitutive androstane receptor; CYP7A1, cholesterol 7α‐hydroxylase; FXR, farnesoid X receptor; GR, glucocorticoid receptor; HNF4, hepatocyte nuclear factor 4; LXR, liver X receptor; MDR3, multidrug resistance protein 3, phospholipid flippase; MRP2, multidrug resistance‐associated protein 2; MRP3, multidrug resistance‐associated protein 3; MRP4, multidrug resistance‐associated protein 4; NTCP, sodium taurocholate cotransporting polypeptide; OSTα/β, organic solute transporter alpha and beta; PC, phosphatidylcholine; PXR, pregnane X receptor; PPARα, peroxisome proliferator‐activated receptor alpha; RAR, retinoic acid receptor; SHP, small heterodimer partner.
Source: Halilbasic et al . [3]. Reproduced with permission of Elsevier.
Hepatocellular transporters are subject to extensive transcriptional and posttranscriptional regulation, allowing for adaptational changes in response to the intracellular accumulation of bile salts. During cholestasis, the NTCP is suppressed through farnesoid X receptor (FXR)‐mediated signaling, thereby preventing the hepatocyte from further accumulating toxic bile salts. Likewise, the expression of OATP1B1 is downregulated. In contrast, cholestasis leads to FXR‐mediated activation of hepatic OATP1B3, which might constitute an escape mechanism promoting the hepatocellular clearance of xenobiotics during cholestasis.
In addition to its role in the uptake of conjugated BAs, NTCP also plays a key role in hepatitis B and hepatitis D virus entry into hepatocytes; and, recently, NTCP has also been shown to modulate hepatitis C virus infection of hepatocytes by regulating innate antiviral immune responses in the liver. As such NTCP has been established as a novel antiviral target.
Apical (Canalicular) Transporters
Various ATP‐binding cassette (ABC) transporters mediate the secretion of bile salts and xenobiotics across the canalicular membrane of hepatocytes. These include members of the family of multidrug resistance (MDR) P‐glycoproteins such as MDR1 (ABCB1), MDR3 (ABCB4), and the bile salt export pump (BSEP or ABCB11). Within the family of MDR proteins, BSEP and MDR3 are two highly conserved members that are involved in the secretion of cholephilic compounds from the liver cell into the bile canaliculus.
BSEP constitutes the predominant bile salt efflux system of hepatocytes and mediates the cellular excretion of numerous conjugated bile salts such as taurine‐ or glycine‐conjugated cholate, chenodeoxycholate, and deoxycholate. MDR3 works as an ATP‐dependent phospholipid flippase, translocating phosphatidylcholine from the inner to the outer leaflet of the canalicular membrane. Canalicular phospholipids are then solubilized by canalicular bile salts to form mixed micelles, thereby protecting cholangiocytes from the detergent properties of bile salts.
In addition to these processes, MRP2, the only canalicular member of the MDR‐associated protein family, mediates the canalicular transport of glucuronidated and sulfated bile salts. MRP2 is the main driving force for bile salt‐independent bile flow through canalicular excretion of reduced glutathione. Furthermore, MRP2 transports a wide spectrum of organic anions, including bilirubin diglucuronide, glutathione conjugates, leukotriene C4, and divalent bile salt conjugates, as well as drug substrates such as chemotherapeutic agents and antibiotics.
MDR1 contributes to the canalicular excretion of drugs and other xenobiotics into bile, although its exact contribution has yet to be established. Its broad substrate specificity and its physiologic expression in various tissues with excretory and protective functions make MDR1 one of the major determinants of drug disposition and toxicity. Substrates are neutral and positively charged organic compounds and include various chemotherapeutic and immunosuppressant agents, antiarrhythmic drugs, HIV protease inhibitors, and antifungals.
Transcriptional regulation of BSEP and MDR3 is mediated by FXR and their activation leads to increased bile salt efflux and the formation of mixed micelles in the biliary tree during cholestatic episodes, thereby preventing the toxic effects of bile salts on hepatocytes and cholangiocytes. In addition, FXR has been shown to induce MRP2 expression, which might constitute another compensatory mechanism during cholestasis. In contrast, MDR1 is upregulated via the pregnane X receptor (PXR), which in addition to endogenous ligands is activated by different xenobiotics. This pathway is part of a general cellular mechanism of detoxification, because MDR1 is the key transporter protein involved in the cellular efflux of numerous drugs and xenobiotics.
Drug Metabolism
The liver has a major role in drug metabolism. The main hepatocyte enzymes involved in metabolism belong to the cytochrome P450 group, a large family of related enzymes housed in the smooth endoplasmic reticulum of the hepatocyte. Metabolism is often divided into two phases of biochemical reaction. Phase 1 involves reduction, hydrolysis or oxidation of the drug, the latter being the most common process. After phase 1 reactions, the resulting drug metabolite is still often chemically active. Phase 2 metabolism involves conjugation with glutathione, methyl or acetyl groups, which usually occurs in the cytoplasm of the hepatocyte and makes the metabolite more hydrosoluble. This facilitates excretion as well as decreasing the pharmacologic activity. Some drugs may undergo just phase 1 or just phase 2 metabolism, but more often the drug will undergo phase 1 and then phase 2 sequentially.
Many factors can affect liver metabolism of drugs. The numbers of hepatocytes and enzyme activity can decline, with a reduction in the metabolic potential of the liver, following aging, acute and chronic liver disease, and conditions that affect hepatic blood flow. Metabolism can also be altered due to genetic deficiency of a particular enzyme and secondary to the use of other drugs as well as dietary and environmental factors. Capillarization of sinusoids during chronic liver disease increases the bioavailability of drugs at high hepatic extraction, possibly increasing the side effects. Drug‐induced liver injury is a major clinical problem, is often favored by exposure to a combination of drugs and, at times, may be mediated by immunologic mechanisms.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Autoimmune Liver Disease»
Представляем Вашему вниманию похожие книги на «Autoimmune Liver Disease» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Autoimmune Liver Disease» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.