Richard Cousley - The Orthodontic Mini-implant Clinical Handbook
Здесь есть возможность читать онлайн «Richard Cousley - The Orthodontic Mini-implant Clinical Handbook» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:The Orthodontic Mini-implant Clinical Handbook
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
The Orthodontic Mini-implant Clinical Handbook: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «The Orthodontic Mini-implant Clinical Handbook»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
provides a thoroughly revised and expanded update to the theoretical and practical aspects of using mini-implants in orthodontic practice. Taking a practical step-by-step approach with hundreds of clinical images, it presents updated clinical techniques and new clinical cases, covering all topics of importance for utilising mini-implants. It also includes a new chapter on mini-implant anchored maxillary expansion appliances.
It begins with a chapter that looks at mini-implant principles and potential complications, before moving onto clinical and design factors for maximising mini-implant success. Other chapters cover incisor retraction; molar distalisation and protraction; intrusion and anterior openbite treatments; bone anchored rapid maxillary expansion; orthognathic surgical uses; and ectopic teeth.
Provides a comprehensive guide to both theoretical and practical advice for the use of mini-implants in orthodontic practice Covers updated clinical techniques and new clinical cases Presents a new chapter on mini-implant anchored maxillary expansion appliances Takes a highly illustrated step-by-step approach ideal for clinical practice
is an essential resource to orthodontists, maxillofacial surgeons, practicing dentists, and anyone with an interest in mini-implant skeletal anchorage.
The Orthodontic Mini-implant Clinical Handbook — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «The Orthodontic Mini-implant Clinical Handbook», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Any irreversible effect from mini‐implant–tooth proximity is on the mini‐implant: it fails (by becoming mobile), not the tooth.
1.11 Perforation of Nasal and Maxillary Sinus Floors
Concerns have been raised in the literature that mini‐implant perforation of the nasomaxillary cavities ( Figure 1.3) may result in either infection or the creation of a fistula. However, the consensus based on dental implant research is that a soft tissue lining rapidly forms over the end of a perforating fixture, and that mini‐implant sites heal by bone infill because of the narrow width of the explantation hole. Motoyoshi et al. [51] investigated clinical effects in a retrospective study where 82 mini‐implants had been inserted mesial and buccal to the maxillary first molar [51]. They found perforation of the maxillary sinus in 10% of the sites, but with no sinusitis symptoms, nor differences in insertion torque and secondary stability. In contrast, a study of infrazygomatic insertions showed that 78% penetrated the maxillary sinus at this site [52]. Whilst these were apparently asymptomatic, mucosal thickening was seen on cone beam computed tomography (CBCT) in 88% of these sites where the mini‐implant penetrated by at least 1 mm. Therefore, in order to maximise bone engagement and minimise both patient discomfort and possible sinus disease, it is generally recommended that maxillary alveolar insertion sites should be within 8 mm of the alveolar crest in dentate areas, and at a more coronal level where maxillary molars are absent. The infrazygomatic crest is not recommended for this reason.
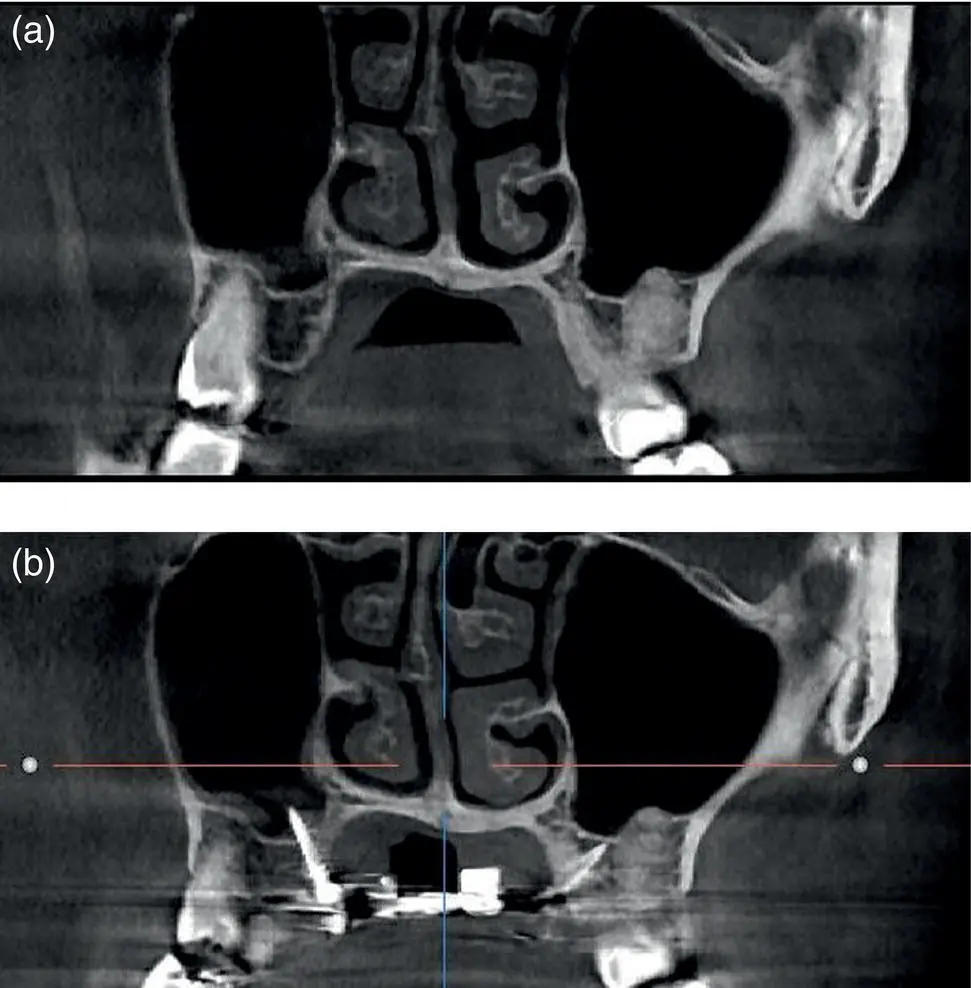
Figure 1.3 Coronal slice views of a CBCT scan of the maxilla (a) before and (b) one month after insertion of mini‐implants in palatal alveolar sites. The mini‐implant, sited distal to the right maxillary first molar, has been inserted at a relatively vertical inclination and has perforated the maxillary sinus, as seen in (b). However, this was asymptomatic and there has been no change in the clarity of the maxillary sinus.
1.12 Damage to Neurovascular Tissues
Disruption of the inferior dental, mental or greater palatine nerves and blood vessels is highly unlikely given their relative distance from standard insertion sites. The nasopalatine nerve is closer to potential anterior palatal insertion sites, but this can be readily avoided if recommended midpalatal insertion procedures are followed; for example, midpalatal insertion sites ought to be distal to the transverse level of the maxillary canines.
1.13 Mini‐implant Fracture
Mini‐implant fracture is thankfully a rare occurrence nowadays since most mini‐implant materials and designs do not easily fracture within the normal torque limits in clinical practice [53,54]. However, some studies, aimed at fracturing mini‐implants in hard acrylic blocks, have failed to allow for the low insertion torques experienced with many designs and especially in the case of self‐drilling body versions. Therefore, fractures due to poor clinical technique may be attributed incorrectly to mini‐implant weakness.
Fracture may occur during insertion, but also on removal if the mini‐implant has been preweakened. Fracture of the mini‐implant tip may occur when a root is inadvertently contacted (i.e. the insertion position and/or angle is incorrect) or when the insertion angle is altered with the mini‐implant partially inserted through the cortical plate. This is most likely to occur due to incorrect technique and/or clinical inexperience. Fracture of the main section of a mini‐implant body is a particular risk, on either insertion or removal, with mini‐implants which feature a narrow diameter and cylindrical body design ( Figure 1.4) [55,56] or when excessive insertion torque occurs (e.g. in the posterior mandible with dense, thick cortical bone). If a mini‐implant fractures on removal, flush with the bone surface, and the retained part is unlikely to impede any remaining tooth movements, then it may be left in situ because of the biocompatibility of titanium alloy ( Figure 1.4c). In the rare event that removal of a fractured part is indicated then this involves creating access by raising a small mucoperiosteal flap, trephination of a narrow collar of bone around the mini‐implant end, and then derotation of the fractured fragment using a Weingarts or mosquitos‐like instrument.
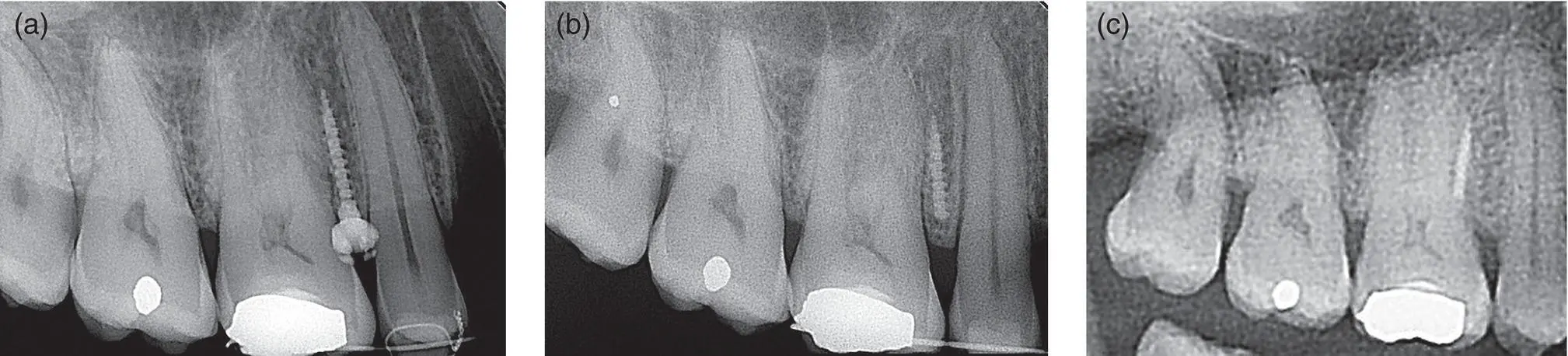
Figure 1.4 Intraoral radiographs taken after (a) insertion of a cylindrically shaped mini‐implant mesial to the maxillary first molar, and (b) its fracture near the coronal end of the body. The initial fracture line is visible in the intact mini‐implant. (c) Sectional orthpantomograph (OPG) showing the (asymptomatic) retained mini‐implant body over five years later.
1.14 Pain
There is often an expectation that high levels of pain will occur but the opposite is true, such that some patients appear to feel virtually no discomfort during and after insertion [57,58]. The majority of patients appear to experience mild pressure‐related pain at the time of insertion and up to 24 hours of low‐level pain thereafter. This is self‐limiting, controlled by simple analgesics (e.g. paracetamol or ibuprofen) and comparable (but of shorter duration) to other orthodontic experiences, such as the effects of separators and aligning archwires [59], and certainly much less than premolar tooth extractions [60]. The latter comparison is beneficial when it comes to explaining the likely pain experience to patients who already have a fixed appliance in situ .
Assuming that the superficial soft tissues have been adequately anaethetised, mini‐implant insertions cause dental pain because of the pressure wave generated by insertion of a rigid fixture into a confined bone space. While there are no pain receptors within the bone tissues, if the pressure dissipates further it will reach the periodontal tissues of adjacent teeth, and hence stimulate their periodontal pain receptors. The patient will feel this as dental pain in the affected tooth. Fortunately, I think that it's within the orthodontist's scope to proactively reduce the level of pressure discomfort by diverging the roots of adjacent teeth prior to insertion (as described in Chapter 5). This creates more interproximal space and hence a greater distance between the mini‐implant site and the adjacent periodontal pain receptors. While there is no clinical evidence to support (or refute) this hypothesis, my experience is that patients with increased interproximal spaces complain of less pain both at the time of insertion and afterwards.
When it comes to mini‐implant removal, local anaesthesia is usually not required and indeed, patients find that the injection sensation is worse than the actual discomfort of explantation [61]. An exception to this rule may occur when a mini‐implant is being removed from the anterior region where there has been some soft tissue overgrowth of the mini‐implant head, especially when it has been inserted in loose mucosa ( Figure 1.5). For all removal procedures, it is essential that the mini‐implant is unwound the entire way out of the implant hole since any attempt to pull it out will result in soft tissue pain where the threads catch on the mucosa. In addition, the orthodontist should ensure that the screwdriver is fully engaged on the mini‐implant at the start of explantation, since premature disengagement during the removal process will cause pain because of the implant's mobility within the soft tissue envelope.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «The Orthodontic Mini-implant Clinical Handbook»
Представляем Вашему вниманию похожие книги на «The Orthodontic Mini-implant Clinical Handbook» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.



Обсуждение, отзывы о книге «The Orthodontic Mini-implant Clinical Handbook» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.