Point-of-Care Ultrasound Techniques for the Small Animal Practitioner
Здесь есть возможность читать онлайн «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Point-of-Care Ultrasound Techniques for the Small Animal Practitioner
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Point-of-Care Ultrasound Techniques for the Small Animal Practitioner: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
New chapters in
cover ultrasound-guided nerve blocks, musculoskeletal, brain imaging, and applications of focused ultrasound techniques in cats, exotics and marine mammals—making it an essential purchase for veterinarians wanting to incorporate point-of-care ultrasound techniques into their veterinary practices.
Presents a standardized approach to point-of-care ultrasound as an extension of the physical exam, including trauma, non-trauma, and monitoring applications Includes coverage of new techniques for focused ultrasound exams, including lung, anesthesia and ultrasound guided nerve blocks, transcranial brain imaging, musculoskeletal, volume status evaluation, and rapid assessment for treatable forms of shock Adds cats, exotic and wildlife mammals, and marine mammals to the existing canine coverage Emphasizes the integration of point-of-care ultrasound techniques for optimizing patient care and accurate patient assessment Offers access to a companion website with supplementary video clips showing many clinically relevant didactic examples The second edition of
is an excellent resource for veterinary practitioners, ranging from the general practitioner to nearly all clinical specialists, including internal medicine, oncology, cardiology, emergency and critical care, anesthesiology, ophthalmology, exotics, and zoo medicine specialists, and veterinary students.
Point-of-Care Ultrasound Techniques for the Small Animal Practitioner — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
What the POCUS Spleen Can Do
Identify focal or multifocal splenic masses or nodules.
Identify parenchymal changes by screening for changes in echogenicity associated with diffuse splenic diseases.
Identify splenic infarction and thrombosis.
Help the clinician to recognize splenic torsion.
These last three goals are inherently more difficult for the novice sonographer and abnormalities should prompt referral for a complete detailed abdominal ultrasound examination.
What the POCUS Spleen Cannot Do
Differentiate benign from malignant splenic masses. The Global FAST approach is a rapid add‐on assessment screening test for localized versus disseminated disease through surveying the abdomen (AFAST), the thorax (TFAST) including heart (TFAST), and lung (Vet BLUE) as well as for detecting other comorbidities.
Definitively diagnose diffuse and localized splenic conditions based on echogenicity.
Reliably determine splenic size (large or small) in dogs (more reliable for size in cats).
Indications
Cranial organomegaly or pendulous abdomen.
Abdominal pain.
Abdominal trauma.
Hematological disorders such as anemia or thrombocytopenia.
Generalized lymphadenopathy.
Episodes of collapse, lethargy or vomiting.
Objectives
Recognize splenic masses (single, multifocal).
Recognize regional and diffuse changes in splenic echogenicity.
Recognize splenic venous congestion, thrombosis, and infarction.
Recognize splenic torsion.
Patient Positioning and Probe Selection
A curvilinear (microconvex) probe is most frequently used to image the spleen, and the MHz is adjusted for the size of the animal. Smaller dogs and cats are generally imaged using higher frequencies of 7.5–10 MHz (less penetration, better detail) and large dogs are generally imaged using lower frequencies such as 5 MHz (deeper penetration, less detail). In small dogs and cats, a linear probe may also be used in order to maximize image quality (due to the higher resolution) when greater penetration depth is not of concern.
Patients are most commonly imaged in dorsal recumbency. In large dogs, however, the cranial aspect of the spleen is often located under the ribcage on the left side. Repositioning these patients into right lateral recumbency allows visualization of the cranial aspect or head of the spleen using a left intercostal approach (Hecht 2008). The authors recommend performing a Global FAST to screen for any intrathoracic problems including pleural and pericardial effusion, cardiac and pulmonary conditions, and abnormal volume status that may pose patient risk before moving the patient into dorsal recumbency.
How to Perform the POCUS Spleen
The patient is placed in dorsal recumbency, the abdomen is shaved, and acoustic coupling gel is applied for best visualization. Although image quality will be diminished, ample application of 70% isopropyl alcohol to haired skin can be utilized in an emergency situation. The spleen is located caudal to the stomach on the patient’s left side and can provide an acoustic window for the left kidney (see also Figures 6.18, 16.3, 16.4, 16.5). The spleen is identified by its hyperechoic (bright white) capsule and blood supply splitting its capsule, unlike the liver. Spleen position and size vary between patients and with the degree of gastric filling. The entire length of the spleen is generally not visualized in one acoustic window and so its entirety must be traced cranially to the head of the spleen and caudally to its tail.
The position of the spleen may vary between patients. The head or cranial aspect of the spleen is generally located on the left side caudal to the last rib. In large dogs, it may be located under the ribcage and therefore, repositioning into right lateral recumbency with a left intercostal approach may be necessary. The spleen is then traced caudally toward its hilus where the splenic vein is imaged and seen branching in a “Y” configuration, referred to by some sonographers as the “whale tail” shaped like the tail fluke ( Figure 9.1; see also Figures 39.8 and 39.9). Splenic arteries are usually not visualized (Hecht 2008). Evaluation of the spleen continues as the sonographer follows the spleen distally along the left side of the abdomen to examine the caudal aspect of the spleen to its tail so that the entire organ has been examined. Remember that the spleen is anchored at the head by its short gastric vessels along the greater curvature of the stomach but has a relatively mobile tail. In some patients, the tail of the spleen may be located medial and to the right side of the patient instead of the left. Several sweeps along the length and width of the spleen may be necessary for a thorough interrogation, especially in animals with splenomegaly.
Pearl:Identify the spleen by its hyperechoic (bright white) capsule and blood supply splitting its capsule, unlike the liver.
Ultrasonographic Findings in a Normal Spleen
When assessing the spleen, systematic evaluation should include the following four features: estimation of size (subjective), evaluation of changes in parenchymal echogenicity, interrogation for mass lesions and nodules, and assessment of splenic vasculature.
Size and Shape
The general contour of the spleen is tongue‐shaped and when viewed adjacent to the left kidney, it appears more triangular (than flat) in cross‐sectional views. Since the size of the spleen can vary in normal animals, estimation of size is generally subjective in dogs except in cases of marked splenomegaly. In cats, splenomegaly is almost always due to pathology and should prompt further evaluation. Spleen thickness greater than 10 mm or a folded spleen invariably indicates splenomegaly in the feline species (Hecht 2008; Reese et al. 2013) ( Figure 9.2; see also Figure 39.9). Benign splenomegaly is uncommon in cats and if present, additional evaluation is warranted.
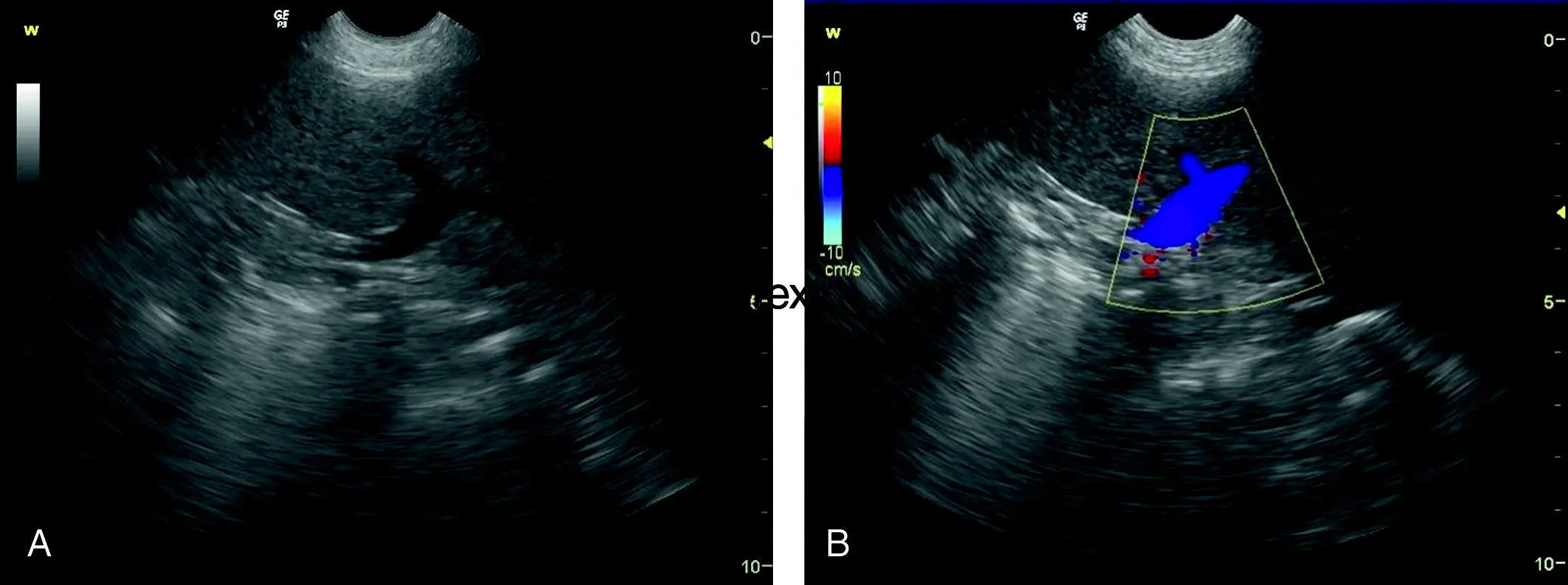
Figure 9.1. Normal splenic hilus. (A) The “Y” shape of the splenic vein, also referred to as the whale tail (mimics tail fluke of the whale), as it branches at the hilus is helpful for identifying the spleen and distinguishing it from the liver. (B) Color flow Doppler may be used to assess blood flow and rule out splenic venous thrombosis and splenic torsion when suspected.

Figure 9.2. Subjective size evaluation of the spleen. Splenic enlargement as evidenced by its folding. The “Y”‐shaped splenic veins departing from its hilus are helpful for identification and distinguishing it from the liver. The spleen here has a homogeneous normal echotexture.
Source: Courtesy of Dr Gregory Lisciandro, DVM, Hill Country Veterinary Specialists and FASTVet.com, Spicewood, TX.
Pearl:Moderate splenomegaly occurs in dogs with many forms of sedation or anesthesia (Hecht 2008; Reese et al. 2013); thus, the effects of sedation and anesthesia must be considered.
Echogenicity
The echogenicity of the splenic parenchyma should be evaluated for diffuse and focal changes. Normal splenic parenchyma is homogeneous in appearance with fine echotexture, and its thin hyperechoic (bright white) capsule may be apparent on long‐axis (sagittal) views. Spleen parenchyma is generally mildly to moderately hyperechoic (brighter) to normal liver parenchyma ( Figure 9.3A,B), and significantly hyperechoic (brighter) to normal renal cortex (Hecht 2008) (see Figure 9.3C,D).
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner»
Представляем Вашему вниманию похожие книги на «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.












Обсуждение, отзывы о книге «Point-of-Care Ultrasound Techniques for the Small Animal Practitioner» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.