Philias R. Garant - Oral Cells and Tissues
Здесь есть возможность читать онлайн «Philias R. Garant - Oral Cells and Tissues» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Oral Cells and Tissues
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Oral Cells and Tissues: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Oral Cells and Tissues»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Oral Cells and Tissues — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Oral Cells and Tissues», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Enamel defects caused by environmental factors are not uncommon. In a study of more than 1,500 schoolchildren in London, it was reported that 68% had enamel defects in the permanent dentition. 164More than 10% had defects on 10 teeth or more.
Genetically acquired enamel defects are much rarer than the environmentally produced varieties. Hereditary enamel dysplasia, also known as amelogenesis imperfecta , occurs in several forms. The hypoplastic form, involving the secretion stage, leads to thin enamel. The teeth are smaller and lack contact points. Exposure of dentin and hypersensitivity are common sequelae. In the hypocalcified or hypomatured type, the enamel is soft, deeply stained, and easily chipped away from the dentin. In general, affected enamel shows an inverse relationship between mineral and protein contents. 165
Amelogenesis imperfecta may be inherited as an autosomal-dominant defect with variable penetrance or as a sex-linked dominant trait. It was recently shown that a mutation in the AMEX gene, deleting nine base pairs in exon 2, resulting in the loss of three amino acids and the exchange of one amino acid in the signal peptide of amelogenin, was sufficient to cause severe enamel hypoplasia ( Fig 3-22). 166In yet another family, a mutation on the AMEX gene, leading to the deletion of a much larger segment (5 kilobases) and the loss of entire exons, caused hypomineralization of enamel ( Figs 3-22and 3-23). 167
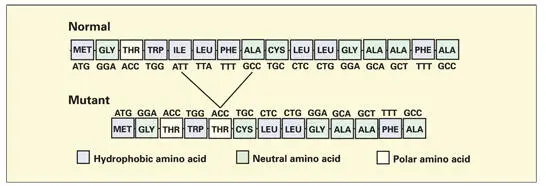
Fig 3-22Base pair and amino acid sequences of normal and mutant signal peptide portions of the human AMEX gene and amelogenin protein. Mutation leading to the loss of a tripeptide (isoleucine, leucine, and phenylalanine) and the substitution of threonine for alanine cause severe hypoplasia. (Adapted from Lagerström-Fermér et al 167with permission.)
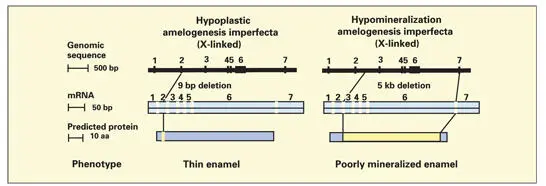
Fig 3-23Two mutations on the AMEX gene that cause amelogenesis imperfecta. (Adapted from Lagerström-Fermér et al 167with permission.)
Enamel pits and fissures
During the development of multicusped teeth, pit and fissure defects are formed in the steep depressions separating adjacent cusps. These defects form when the enamel organ is compressed by the growth of enamel along the slope of the cusps, constricting the ameloblasts that are located in the deepest and most narrow regions of the depression ( Fig 3-24). Degeneration of the ameloblasts results in the formation of a pit and/or fissure running from the surface of the crown to a level just above the dentin. A thin layer of enamel at the base of the defect is usually formed by the ameloblasts prior to their death. The space created by the degeneration of the cells of the enamel organ provides a niche that becomes colonized by bacteria as soon as the tooth erupts into the mouth.
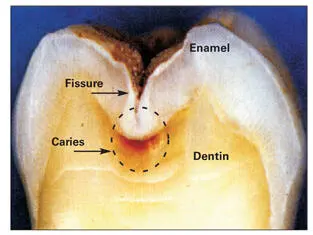
Fig 3-24Mineralized tooth sectioned in half to reveal caries in the enamel (chalky white) along the sides of a fissure and below it in the dentin (brownish red). (From Paterson et al. 172Reprinted with permission.)
Pits and fissures are the parts of the tooth most susceptible to caries attack. Acid production by bacteria demineralizes adjacent enamel and dentin, leading to the formation of an incipient carious lesion (see Fig 3-24). Because the amount of enamel at the floor of the defect is minimal, the caries process can invade the dentin within a short time after its initiation. Unless teeth are protected with fluoride or an occlusal sealant, there is a very high probability that they will develop clinically detectable pit and fissure caries within 2 years after eruption.
Infant malnutrition and dental disease
A growing body of evidence accumulated during the past two decades has established the importance of an adequate intake of protein during early childhood for optimal dental health. Protein malnutrition during the formative years leads to delay of tooth eruption and increased susceptibility to dental caries later in life. 168, 169The combination, frequently found in underdeveloped countries, of protein malnutrition in infants and subsequent increased consumption of sucrose-containing foods by children and adolescents, leads to a widespread incidence of dental caries.
Although the specific underlying biochemical deficiencies in enamel and dentin matrix that result from insufficient consumption of dietary protein remain to be established, it is clear that ameloblasts and odontoblasts require high levels of energy as well as a wide variety of amino acids for protein synthesis. Thus they are detrimentally affected in periods of protein starvation. Furthermore, enamel matrix produced during embryonic development and early childhood cannot undergo subsequent remodeling. Therefore, any deficiency occurring during its development will lead to increased susceptibility to dental disease in later life.
Fluoride, dental caries, and fluorosis
Epidemiologic studies conducted nearly a half-century ago demonstrated an inverse relationship between the level of fluoride in local water supplies and caries experience. Children who grew up in communities with fluoride levels greater than 1.0 ppm in drinking water experienced significantly fewer dental caries than did children in neighboring towns with low fluoride concentrations (less than 0.5 ppm) ( Fig 3-25). 170
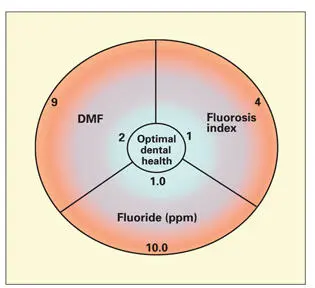
Fig 3-25Relationship between fluoride levels in drinking water (in parts-per-million [ppm]), the detrimental effects of high fluoride intake (fluorosis index), and dental health as measured by the number of diseased, missing, and filled teeth (DMF). (Adapted from Shaw et al. 170)
Fluoride enters hydroxyapatite mineral, where it substitutes for hydroxyl ions. Incorporation of fluoride into enamel and dentin occurs during tooth development. Additional fluoride is added even after enamel maturation, as fluoride is absorbed in surface enamel from tissue fluids prior to eruption and from saliva once the teeth have erupted into the oral cavity. Fluoridated hydroxyapatite is more resistant to acid demineralization than is nonsubstituted mineral. The addition of only small amounts of fluoride to the hydroxyapatite crystal greatly improves its stability by decreasing the mobility of hydroxyl ions within the crystal lattice. 171
The addition of fluoride in drinking water supplies at the optimal level of 1.0 ppm has a great dental health benefit, reducing the incidence of dental caries by more than 50%. Furthermore, the reduction in dental caries minimizes other pathologic sequelae that result from early tooth loss.
High levels of fluoride consumed during the period of tooth development have detrimental effects on enamel formation (see Fig 3-25). Sustained consumption of fluoride at levels greater than 4.0 ppm causes dental fluorosis, a condition characterized by chalky white defects and areas of yellow-brown discoloration in the enamel. Chronic ingestion of fluoridated toothpaste or mouthrinse in areas with optimally fluoridated water can raise systemic fluoride concentrations to a level at which fluorosis may develop. Despite the enamel defects, the involved teeth are more resistant to caries. For the patient, enamel fluorosis is mainly an esthetic problem.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Oral Cells and Tissues»
Представляем Вашему вниманию похожие книги на «Oral Cells and Tissues» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.





Обсуждение, отзывы о книге «Oral Cells and Tissues» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.