Digital Workflow in Reconstructive Dentistry
Здесь есть возможность читать онлайн «Digital Workflow in Reconstructive Dentistry» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Digital Workflow in Reconstructive Dentistry
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Digital Workflow in Reconstructive Dentistry: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Digital Workflow in Reconstructive Dentistry»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Contributors
Amirah M. R. Alammar • Abdulaziz Alsahaf • Wael Att • Maria Bateli • Jasmin Bernhart • Shaza Bishti • Sarah Blattner • Miha Brezavšček • Sandy Cepa • Nadine Emmanoulidi • Ahmed Fawzy • Manrique Fonseca • Michele Frapporti • Rumpa Ganguly • Yousef Al-Ghamdi • Petra Ch. Gierthmuehlen • Aiste Gintaute • Ulrich Lamott • Christos Lamprinos • Matthias Petsch • Udo Plaster • Aikaterini Ploumaki • Hanna Rauberger • Elisabeth Schwartzkopff • Christian F. Selz • Thamer Al-Sharif • Benedikt Spies • Frank A. Spitznagel • Jörg R. Strub • Michael Swain • Taskin Tuna • Alexander Vuck • Siegbert Witkowski
Digital Workflow in Reconstructive Dentistry — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Digital Workflow in Reconstructive Dentistry», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Typically, the processing/planning software can be used for analysis and diagnostics (e.g., caries and lesion detection), treatment planning (virtual mock-up, virtual implant treatment planning, virtual orthodontics treatment planning, and so on), or CAD. In terms of caries and lesion detection, several companies are working now on introducing AI for automatic detection of caries as well as further pathological lesions from radiographs, namely periapical radiographs, panoramic radiographs, or CBCT. Also, AI is being implemented for automatic annotation of different anatomical structures, such as mandibular nerve, impacted teeth, maxillary sinus, floor of the nose, and others. Likewise, there are undergoing developments to enable automatic detection and segmentation of the teeth from CBCT and creation of separate files (STLs) of the teeth, as well as the bony structures. The implementation of such technologies in the near future will accelerate the workflow and enhance the diagnostic experience for the clinician, thus providing a better healthcare service for the patient.
Data processing/planning software for treatment planning is one of the most important components of the digital workflow. It is not only intended for communication between the patient and the treatment team, but also an important tool for treatment planning and expectations. A good example is implant planning software, where CBCT data (typically DICOM files) is imported into the software and used to plan the implant position virtually with consideration of the anatomical structures as well as the restorative needs. Another application is the use of patient facial photographs in combination with calibrated intraoral scan or model scan data to analyze and plan the future esthetic rehabilitation (e.g., smile design software) in terms of tooth length, width, and proportions, as well as shade, and share the information with the patient as well as the treatment team. While such features facilitate design capabilities, CAD is considered the last component of data processing/planning. Here, the software is used to design the form of the intended object (e.g., crown, prosthesis, surgical guide, night guard, virtual wax-up, and so on) before moving to the last component of the digital workflow.
Execution of Treatment or Fabrication
The last component of the digital workflow is to perform the planned treatment or production of the intended object by means of computer-aided manufacturing (CAM). CAD data is imported into CAM software, where details of the production process can be simulated and executed (e.g., placement of supportive structures or simulation of the milling/grinding process). Both the subtractive and the additive manufacturing technologies are available for CAM.
The subtractive technologies can be subcategorized into milling and grinding. It is considered as the most widely spread manufacturing technology. The manufacturing machines can be divided into chairside or lab units. In the former option, the unit is typically intended for the manufacture of single-unit restorations during the same office visit. For a larger-scale production and more demanding units/restorations, the latter option is selected. The milling machine can be either in an office, a laboratory, or a central manufacturing facility. On the other hand, additive manufacturing is becoming increasingly popular. Here, several methods are available for manufacturing of an object, including but not limited to selective laser sintering (SLS), digital light processing (DLP), stereolithography (SL), and three-dimensional printing (3D printing). The latter technology is considered to be the most up to date and improving day by day. However, the scientific evidence about its accuracy and efficiency is still limited. Comparatively, the other additive manufacturing technologies are well established. For example, SL is considered for a long time as the method of choice for central manufacture of surgical guides or models with a predictable accuracy. Also, SLS is being used to produce nonprecious alloy frameworks of crowns and fixed partial dentures with a predictable accuracy. While many techniques already exist, significantly further technologies and materials for additive manufacturing are expected to be introduced within the next few years. Further details about the different CAM technologies are provided in Chapter 10.
References
1.Att W, Gerad M. Digital workflow in reconstructive dentistry: new technologies for high-strength ceramics. In: Ferenz J, Navarro J, Silva N (eds). High-Strength Ceramics. Chicago, IL: Quintessence Publishing, 2014.
Introduction
The evolution of computer-aided impression-making occurred almost simultaneously with major developments in dental computer-aided design/computer-aided manufacturing (CAD/CAM). In the 1970s, dentists John Young and Bruce Altschuler first attempted to introduce CAD/CAM technology into dentistry, developing an intraoral grid mapping system using an optical apparatus. 1Dr. Francois Duret developed and patented the first CAD/CAM device in 1984. 2-4Two years later, at the Chicago Midwinter Meeting in 1989, the device, called Sopha System (Sopha Bioconcept, CA, USA), was officially and publicly launched. During this meeting, a crown fabrication was demonstrated and it took four hours to be completed. 5Prior to crown design and milling, an optical impression of an abutment tooth had been performed. The optical impression could be obtained either extraorally from a dental casting gypsum model, or intraorally by a 512 × 512 pixel charge-coupled device (CCD) camera, using a method derived from electronic Moiré patterns. 3,6Several factors, such as complexity and cost, impeded the success of the system in the dental market. 3,7In 1980, Dr Werner Mörmann and an electrical engineer, Marco Brandestini, developed a CAD/CAM system that was introduced in 1987 as Cerec (Chairside Economical Restoration of Esthetic Ceramics) by Sirona Dental Systems, Bensheim, Germany. At that time, Cerec was considered the first commercially available CAD/CAM system for the fabrication of dental restorations that utilized a compact intraoral 256 × 256 pixel CCD camera for data acquisition. 4,8,9The NobelProcera system (Nobel Biocare, Gothenburg, Sweden) was developed by Dr Matts Andersson as a result of his efforts to fabricate titanium copings. The data for the CAD/CAM process was obtained from a stone cast (master die) via digitizing by means of a tactile scanning device. 10,11
The developers of Cerec have set as a goal the proper functional, biological, and esthetic prosthetic restoration of teeth within a single visit. 12Its introduction enabled the fabrication of inlays, while later versions, Cerec II and III, facilitated the fabrication of onlays and single crowns. Since 2005, several other intraoral scanners (IOSs) with improved features have been introduced into the market ( Fig 2.1). In recent years, the market of IOS systems has been grown increasingly with the introduction of new devices as well as developments to existing systems ( Fig 2.2, Table 2.1).

Fig 2.1Overview of the currently available and most frequently used IOS systems.
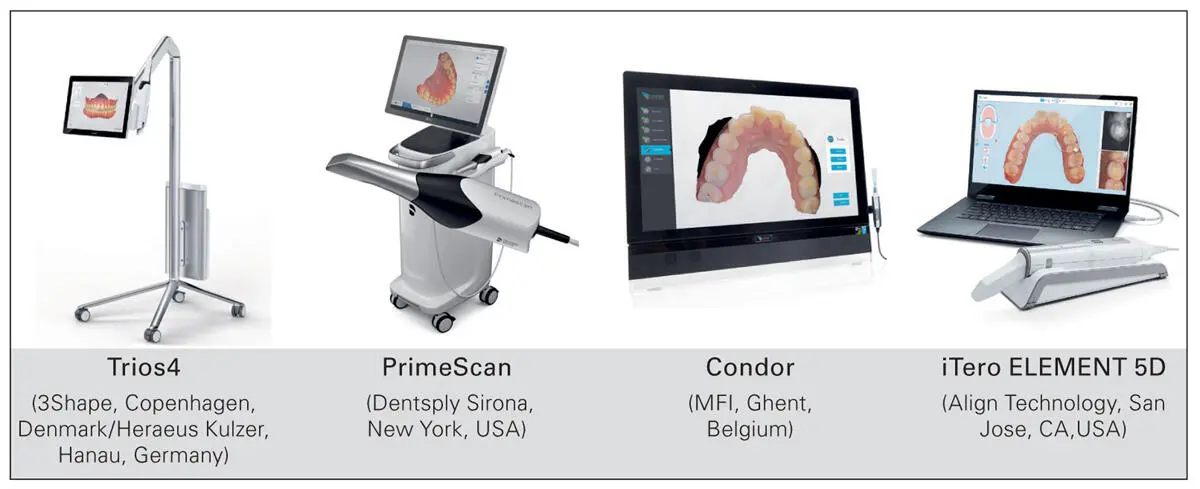
Fig 2.2Several commercially available IOS systems. With new models, the device’s footprint is becoming significantly smaller.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Digital Workflow in Reconstructive Dentistry»
Представляем Вашему вниманию похожие книги на «Digital Workflow in Reconstructive Dentistry» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Digital Workflow in Reconstructive Dentistry» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.