Clinical Pancreatology for Practising Gastroenterologists and Surgeons
Здесь есть возможность читать онлайн «Clinical Pancreatology for Practising Gastroenterologists and Surgeons» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Clinical Pancreatology for Practising Gastroenterologists and Surgeons
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Clinical Pancreatology for Practising Gastroenterologists and Surgeons: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Clinical Pancreatology for Practising Gastroenterologists and Surgeons»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
was first published sixteen years ago, the knowledge and clinical management of pancreatic diseases have developed markedly. Thanks to the development of translational research and the “from bench to bedside” concept, much progress from the lab has been applied to clinical practice. Additionally, several highly relevant clinical trials published over the last decade have resulted in the updating and optimisation of clinical guidelines.
A new and validated classification of the severity and complications of acute pancreatitis that is firmly rooted in clinical practice has become the basis for the development of minimally invasive approaches to pancreatic necrosis. The etiopathogenic knowledge of chronic pancreatitis and other pancreatopaties, like that associated with diabetes mellitus, has developed significantly. Increased study of cystic pancreatic tumours, which has been reflected in the publication of several guidelines and consensus reports over the last few years, is especially important. Most research efforts have focused on pancreatic cancer, which have led and will further lead to a significant increase in the therapeutic armamentarium against this devastating disease. Finally, many newly published studies have changed the concept, causes, clinical relevance, diagnosis and treatment of exocrine pancreatic insufficiency. Updates based on these developments and more are included in the new edition of
.
This new edition of
is a result of the collaboration between the world's leading experts in each area of clinical pancreatology, with the aim of facilitating gastroenterologists, surgeons, oncologists, internists, nutritionists, diabetologists, paediatricians, radiologists, pathologists and other specialists in their daily clinical practice. This book is an indispensable update providing leading knowledge in clinical pancreatology.
Clinical Pancreatology for Practising Gastroenterologists and Surgeons — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Clinical Pancreatology for Practising Gastroenterologists and Surgeons», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
The technique is always performed under general anesthesia. It consists of a conventional exploratory laparoscopy with three or four ports, reaching the pancreatic lodge to complete the necrosectomy and inserting large‐caliber drains in order to continue with postoperative lavages. The preferred route for accessing the pancreatic cell is via the gastrocolic ligament and greater omentum ( Figure 15.3). In a variant of this technique, a device is used for hand‐assisted surgery (GELport) to allow necrosectomy by digital blunt dissection.
Laparoscopic transgastric necrosectomy is a particular variant of this approach. This technique follows the same principle as endoscopic necrosectomy but uses a laparoscopic approach. WON located retrogastrically is deemed to be ideal for this approach, given its close contact with the gastric posterior wall [35].
The patient is placed in the decubitus position and intervention is carried out under general anesthesia. Entry into the peritoneal cavity and ports are the same as the previously described intervention and gastrotomy is performed ( Figure 15.4b) at the level of the necrosis located by intraoperative ultrasonography. Needle aspiration is performed for both anatomical confirmation and to obtain intraoperative cultures ( Figure 15.4c). A wide posterior necrosectomy is then performed by electrocautery to access the necrotic tissue. Blunt debridement of the necrosis is carried out ( Figure 15.4d) and as much as possible of the necrotic debris is removed directly. The posterior gastrotomy is left open to drain the necrotic cavity and the anterior wall gastrotomy is closed by an intracorporeal suture.
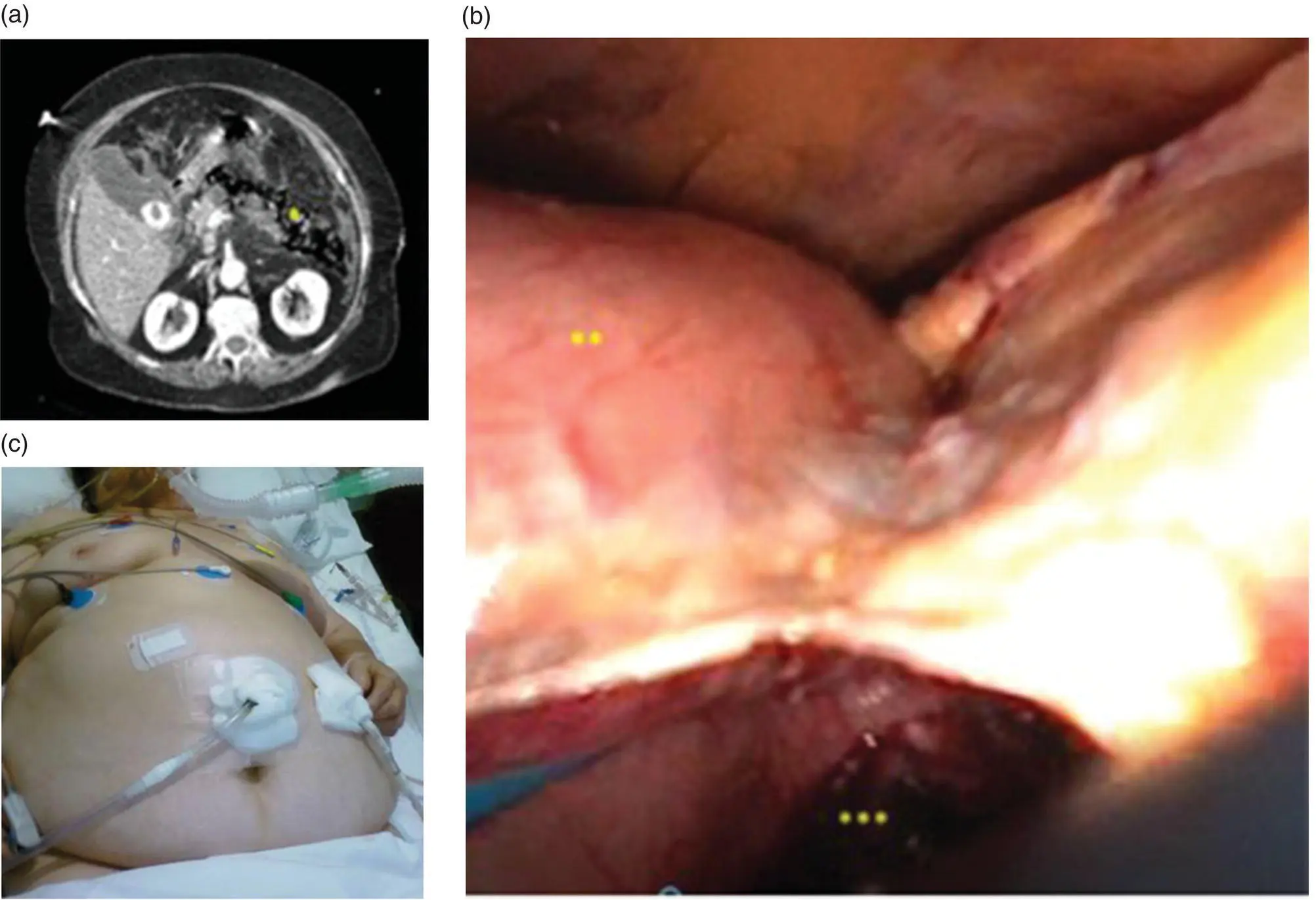
Figure 15.3 Laparoscopic transperitoneal approach. (a) Location of the necrosis by CT scan. (b) Necrosis is reached via the gastrocolic ligament and greater omentum. (c) Drains are placed as shown. *, Peripancreatic retropneumoperitoneum; **, greater curvature of the stomach; ***, pancreatic necrotic collection.
Source: courtesy of Patricia Sánchez‐Velázquez.
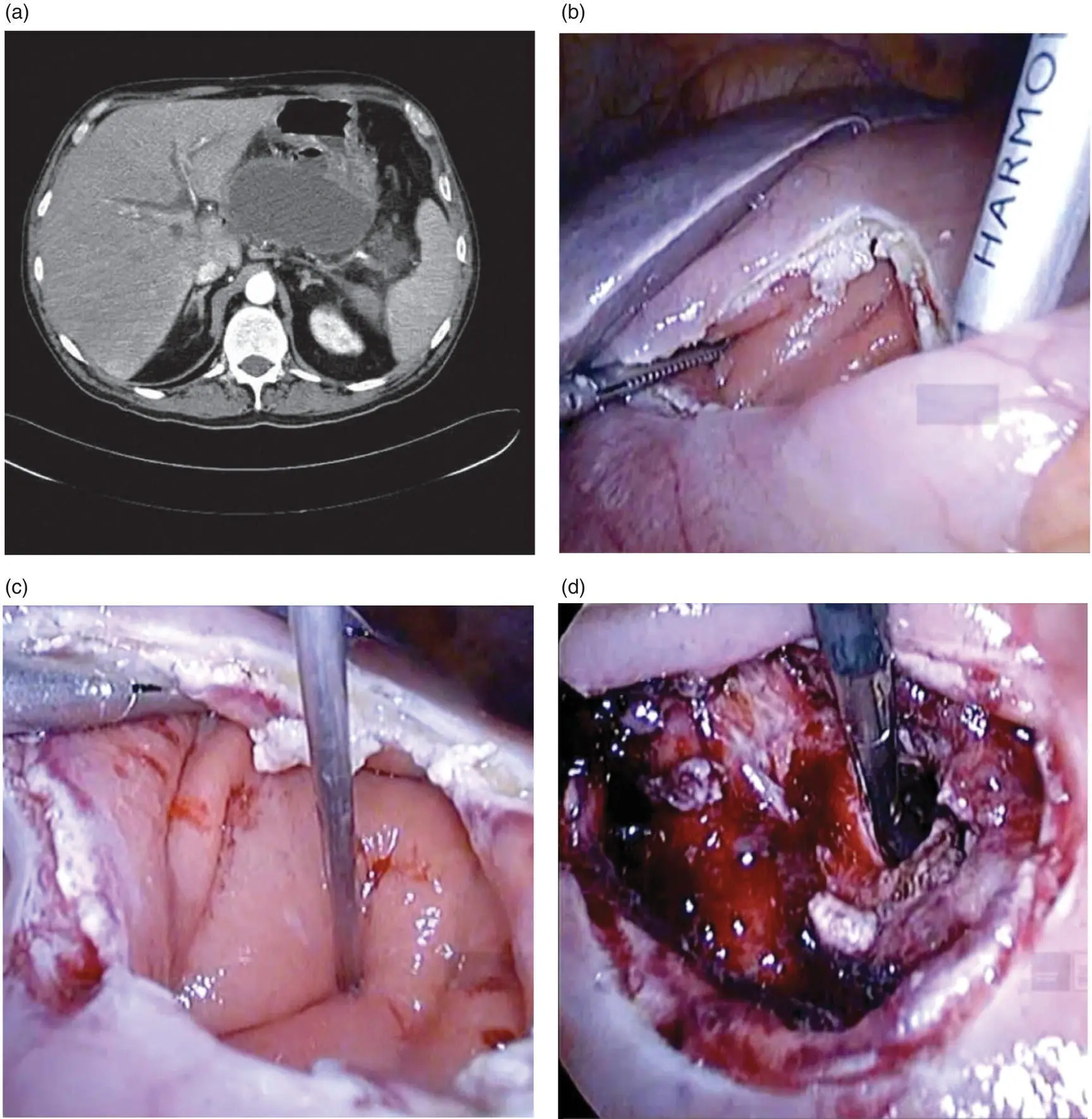
Figure 15.4 Laparoscopic transgastric necrosectomy. (a) CT scan diagnoses a retrogastrically placed walled‐off necrosis. (b) Gastrotomy with harmonic device. (c) Location of the necrosis by punction. (d) Necrosis drained by dividing the posterior gastric wall.
Source: courtesy of Patricia Sánchez‐Velázquez.
Although there is not enough robust data to recommend this technique over the others, it does have some advantages in that it overcomes the limitations of endoscopic necrosectomy, such as a lower cost than lengthy treatments with repeated interventions.
References
1 1 Allardyce DB. Incidence of necrotizing pancreatitis and factors related to mortality. Am J Surg 1987; 154(3):295–299.
2 2 Fernndez‐Cruz L, Beger HG. Surgical approaches to acute necrotizing pancreatitis. In: Domínguez Muñoz JE (ed.) Clinical Pancreatology for Practising Gastroenterologists and Surgeons. Oxford: Blackwell Publishing, 2005:133–140.
3 3 Büchler MW, Gloor B, Müller CA, et al. Acute necrotizing pancreatitis: treatment strategy according to the status of infection. Ann Surg 2000; 232(5):619–626.4.Besselink MG, De Bruijn MT, Rutten JP, et al. Surgical intervention in patients with necrotizing pancreatitis. Br J Surg 2006; 93(5):593–599.
4 5 Rau B, Uhl W, Buchler MW, Beger HG. Surgical treatment of infected necrosis. World J Surg 1997; 21(2):155–161.
5 6 Mier J, Luque‐De León E, Castillo A, et al. Early versus late necrosectomy in severe necrotizing pancreatitis. Am J Surg 1997; 173(2):71–75.
6 7 Besselink MGH, Verwer TJ, Schoenmaeckers EJP, et al. Timing of surgical intervention in necrotizing pancreatitis. Arch Surg 2007; 142(12):1194–1201.
7 8 Uhl W, Warshaw A, Imrie C, et al. IAP guidelines for the surgical management of acute pancreatitis. Pancreatology 2002; 2(6):565–573.
8 9 Johnson CD, Sarr MG, Tsiotos GG, et al. Classification of acute pancreatitis – 2012: revision of the Atlanta classification and definitions by international consensus. Gut 2012; 62(1):102–111.
9 10 Traverso LW, Kozarek RA. Pancreatic necrosectomy: definitions and technique. J Gastrointest Surg 2005; 9(3):436–439.
10 11 Beger HG, Rau B. Necrosectomy and postoperative local lavage in necrotizing pancreatitis. Ann Ital Chir 1995; 66:209–215.
11 12 Ashley SW, Perez A, Pierce EA, et al. Necrotizing pancreatitis: contemporary analysis of 99 consecutive cases. Ann Surg 2001; 234(4):572–580.
12 13 Raraty MGT, Halloran CM, Dodd S, et al. Minimal access retroperitoneal pancreatic necrosectomy. Ann Surg 2010; 251(5):787–793.
13 14 van Santvoort HC, Besselink MG, Bakker OJ, et al. A step‐up approach or open necrosectomy for necrotizing pancreatitis. N Engl J Med 2010; 362(16):1491–1502.
14 15 Petrov MS, Shanbhag S, Chakraborty M, et al. Organ failure and infection of pancreatic necrosis as determinants of mortality in patients with acute pancreatitis. Gastroenterology 2010; 139(3):813–820.
15 16 Bradley EL. A clinically based classification system for acute pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga, September 11 through 13, 1992. Arch Surg 1993; 128(5):586–590.
16 17 Freeny PC, Hauptmann E, Althaus SJ, et al. Percutaneous CT‐guided catheter drainage of infected acute necrotizing pancreatitis: techniques and results. AJR Am J Roentgenol 1998; 170(4):969–975.
17 18 Bello B, Matthews JB. Minimally invasive treatment of pancreatic necrosis. World J Gastroenterol 2012; 18(46):6829–6835.
18 19 Van Baal MC, Van Santvoort HC, Bollen TL, et al. Systematic review of percutaneous catheter drainage as primary treatment for necrotizing pancreatitis. Br J Surg 2011; 98(1):18–27.
19 20 van Grinsven J, van Dijk SM, Dijkgraaf MG, et al. Postponed or immediate drainage of infected necrotizing pancreatitis (POINTER trial): study protocol for a randomized controlled trial. Trials 2019; 20(1):239.
20 21 Poves I, Burdío F, Dorcaratto D, Grande L. Minimally invasive techniques in the treatment of acute biliary pancreatitis. Central Eur J Med 2013; 60(Suppl 7):13–19.
21 22 Carter CR, McKay CJ, Imrie CW. Percutaneous necrosectomy and sinus tract endoscopy in the management of infected pancreatic necrosis: an initial experience. Ann Surg 2000; 232(2):175–180.
22 23 Goenka MK, Goenka U, Mujoo MY et al. Pancreatic necrosectomy through sinus tract endoscopy. Clin Endosc 2018; 51(3):279–284.
23 24 Bakker OJ, van Santvoort HC, van Brunschot S, et al. Endoscopic transgastric vs surgical necrosectomy for infected necrotizing pancreatitis: a randomized trial. JAMA 2012; 307(10):1053–1061.
24 25 Baron TH, Thaggard WG, Morgan DE, Stanley RJ. Endoscopic therapy for organized pancreatic necrosis. Gastroenterology 1996; 111(3):755–764.
25 26 Escourrou J, Shehab H, Buscail L, et al. Peroral transgastric/transduodenal necrosectomy. Ann Surg 2008; 248(6):1074–1080.
26 27 van Brunschot S, van Grinsven J, van Santvoort HC, et al. Endoscopic or surgical step‐up approach for infected necrotising pancreatitis: a multicentre randomised trial. Lancet 2018; 391(10115):51–58.
27 28 Gambiez LP, Denimal FA, Porte HL, et al. Retroperitoneal approach and endoscopic management of peripancreatic necrosis collections. Arch Surg 1998; 133(1):66–72.
28 29 Horvath KD, Kao LS, Wherry KL, et al. A technique for laparoscopic‐assisted percutaneous drainage of infected pancreatic necrosis and pancreatic abscess. Surg Endosc 2001; 15(10):1221–1225.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Clinical Pancreatology for Practising Gastroenterologists and Surgeons»
Представляем Вашему вниманию похожие книги на «Clinical Pancreatology for Practising Gastroenterologists and Surgeons» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.












Обсуждение, отзывы о книге «Clinical Pancreatology for Practising Gastroenterologists and Surgeons» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.