Fernando Suarez - Periodontics
Здесь есть возможность читать онлайн «Fernando Suarez - Periodontics» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Periodontics
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Periodontics: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Periodontics»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Periodontics — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Periodontics», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Early experimental studies evaluated the potential of radiographs to detect periodontal bony defects using human cadaver skulls. 95–102Prichard was the first to describe a “subtle shadow” in radiographs pointing toward the opening of the mesial furcation of maxillary first molars. 99Then, Hardekopf et al coined the term furcation arrowand defined it as a radiographic shadow associated with a proximal furcation involvement. 8Using skulls with furcation-involved molars, authors reported a significant association of Degree II and III furcation defects with the presence of furcation arrows in both mesial and distal furcation entrances when compared to noninvolved molars. For Degree I defects and noninvolved furcations, the incidence of furcation arrows was low and insignificant. Nonetheless, it was concluded that the absence of a furcation arrow does not necessarily mean an absence of a furcation involvement. 8
Overall, the usefulness of the furcation arrow as a diagnostic marker is limited. When detected on radiographs, these can predict furcation involvements only in 70% of cases; yet, furcation arrows were also seen in less than 40% of sites with truly present furcation involvement. Consequently, the furcation arrow has a sensitivity of 38.7%, a specificity of 92.2%, a positive predictive value of 71.7%, and a negative predictive value of 74.6%. 100
Currently, a combination of both clinical and conventional radiographic assessments remains as the gold standard approach for detecting furcation defects. Limited evidence supports the use of CBCT for periodontal disease diagnosis. 101–103
Root Morphology
ROOT SURFACE AREA
Root surface areahas been extensively explored in the literature ( Table 5-6). 104–108While initially investigated as an important factor to aid clinicians in decision making for root resection therapy, 13the calculation of this area is also helpful to determine the extent of disease progression and to assist in the selection between regenerative or resective approaches.
TABLE 5-6 Average root surface area (mm 2) covered by cementum *
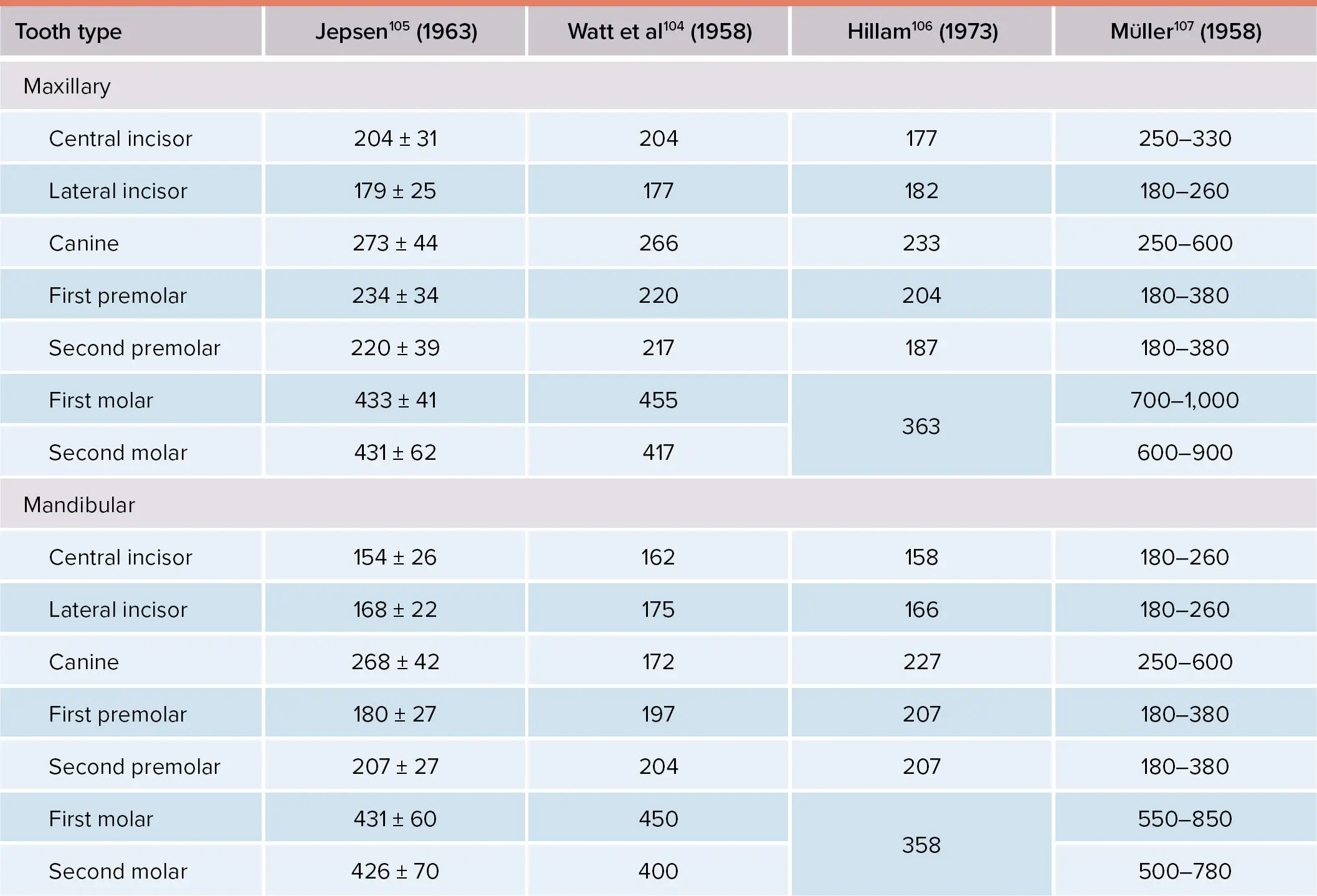
*Adapted from Schroeder. 108
Hermann et al 13reported a total surface area for the maxillary first molar of 476.43 mm 2. Interestingly, the authors went further to investigate the percentage of root surface area occupied by root trunk (32%), palatal (24%), mesiobuccal (25%), and distobuccal (19%) roots (Fig 5-3a). Later, similar studies were conducted around mandibular first molars. 69,109Dunlap and Gher reported a total surface area of 436.8 mm 2, and the percentage of root surface area for the root trunk, distal, and mesial root were 30.5%, 32.4%, and 37%, respectively 69(Fig 5-3b). Box 5-3includes a summary for the percentages of root surface area for each region in the root complex. 13,68

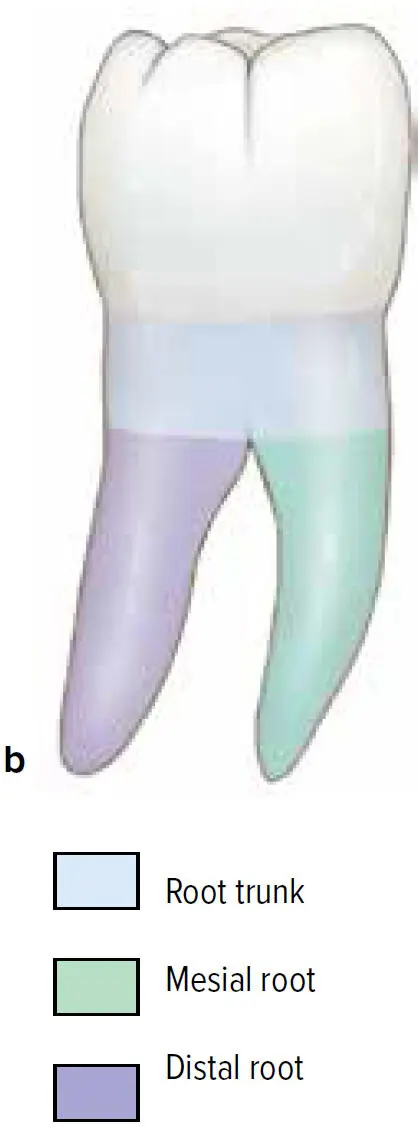
Fig 5-3 Percentage of root surface area of maxillary (a) and mandibular (b) first molars.
BOX 5-3 Percentage of root surface area in the root complex
| Maxillary first molars(Hermann et al 13) | Mandibular first molars(Gher and Dunlap 68) | ||
| Root trunk | 32% | Mesial root | 37% |
| Mesiobuccal root | 25% | Distal root | 32.4% |
| Palatal root | 24% | Root trunk | 30.5% |
| Distobuccal root | 19% |
ROOT CONCAVITIES
Root concavitiesare common features of the root configuration and act as predisposing sites for periodontal breakdown. 70Additionally, the presence of these developmental depressions will impair mechanical instrumentation during nonsurgical and surgical therapy, especially for multirooted teeth.
Fox and Bosworth conducted a morphologic assessment to determine the presence of proximal concavities on extracted teeth among all tooth types. 110The authors concluded that nearly every tooth has concavities at or within 5 mm apical to its CEJ. 110For multirooted teeth specifically, Booker and Loughlin reported mesial concavity depths of 0.35 mm and 0.44 mm associated with single-rooted and two-rooted maxillary first premolars, respectively. 74Generally, these depressions tend to be deeper on the mesial aspects and middle third of the root surface. 75Conversely, Gher and Vernino reported a prevalence of 78% of concavities around maxillary premolars being not clinically relevant until 50% of interproximal bone loss had occurred. 70
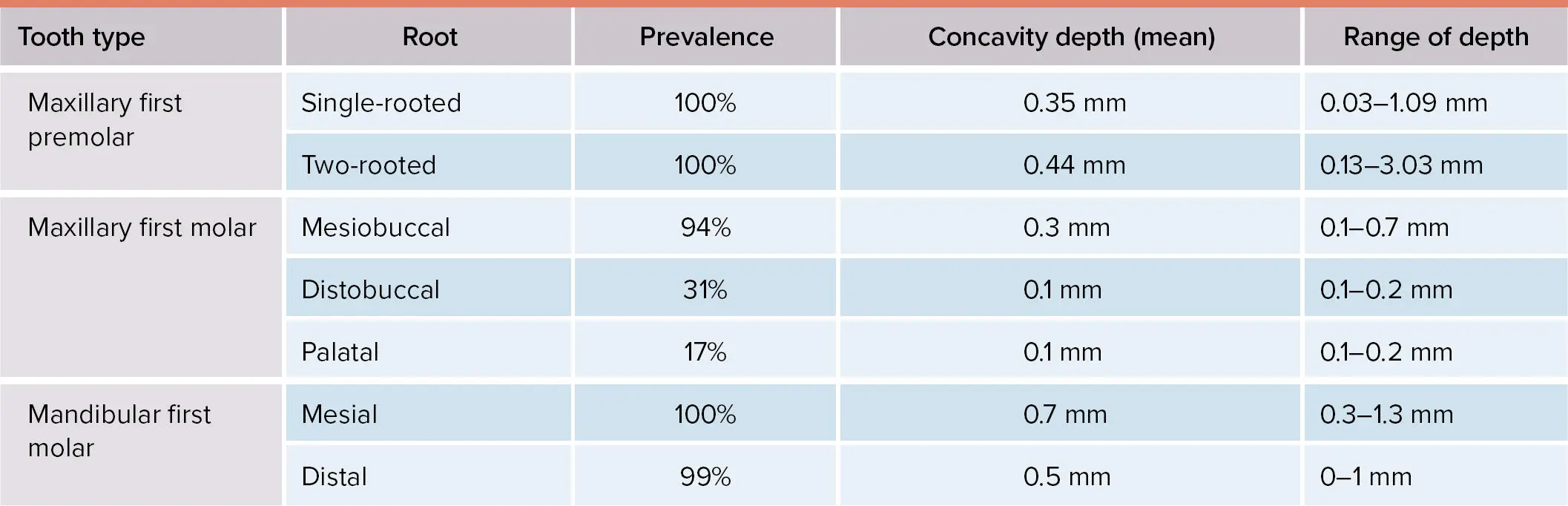
Bower also extensively explored the concavity depth and incidence around maxillary and mandibular first molars. 111Within the maxillary first molar, concavities are more likely found on mesiobuccal (94%) than distobuccal (31%) or palatal (17%) root surfaces. A higher incidence was also noted among mandibular first molars on both mesial (100%) and distal (99%) root surfaces ( Table 5-7). 74,111
TABLE 5-7 Prevalence and root concavity depth around maxillary and mandibular molars 74,111
Root Proximity
DEFINITION AND CHARACTERISTICS
Root proximityhas been defined as interradicular distances (IRDs) of less than or equal to 0.8 mm or less than 1 mm presenting as a risk marker for periodontal disease. 112–119In a classic study, Heins and Wieder examined the nature of IRD spaces using human histology and reported a distance ranging from 0.2 to 4.5 mm between second premolars, first molars, and second molars. 120Interestingly, sites exceeding 0.5 mm (89.6%) of IRD showed signs of cancellous bone flanked by lamina dura. When this distance is less than 0.5 mm, a fused lamina dura was observed with no signs of cancellous bone in between. Ultimately, sites with less than 0.3 mm of IRD were connected only by the PDL ( Table 5-8). 120
TABLE 5-8 Histologic features based on IRD 120
| Interradicular distance | Histologic features |
| ≥ 0.5 mm | Cancellous bone, lamina dura, and PDL |
| < 0.5 mm | Lamina dura and PDL |
| < 0.3 mm | Only PDL |
Vermylen et al reported a 15.3% prevalence of root proximity among 5,122 interproximal sites from 197 patients. 113It is important to note that 68% of sites were located affecting primarily maxillary molars as well as central and lateral mandibular incisors. 113In a case control study, root proximity was encountered more often at the coronal and middle thirds of the root. 115Moreover, sites with bilateral root proximity had 3.6 times greater risk of developing periodontitis. Similarly, Kim et al examined 473 patients with a mean follow-up time of 23 years to evaluate the association between root proximity and the risk for alveolar bone loss. 119The mean IRD and alveolar bone loss was 1.0 mm and 0.61 mm, respectively. Sites with less than 0.6 mm of IRD presented an increased risk for alveolar bone loss than those with 0.8 mm or more, especially in mandibular anterior teeth.
Similarly, a higher risk for occurrence of intrabony defects has been associated with IRD between 2.1 to 4.1 mm. 121Trossello and Gianelly reported more bone loss at sites with less than 1 mm of root proximity (13.4%) and in patients who had received orthodontic treatment. 112On the other hand, Årtun et al examined 400 patients who completed orthodontic treatment with at least a 16-year follow-up. Among them, 25 patients (6%) with root proximity had no significant differences regarding inflammation, attachment level, and bone level in comparison with neighboring control sites. 122
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Periodontics»
Представляем Вашему вниманию похожие книги на «Periodontics» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.




Обсуждение, отзывы о книге «Periodontics» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.