Ron Ben-Amotz - Complications in Canine Cranial Cruciate Ligament Surgery
Здесь есть возможность читать онлайн «Ron Ben-Amotz - Complications in Canine Cranial Cruciate Ligament Surgery» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Complications in Canine Cranial Cruciate Ligament Surgery
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Complications in Canine Cranial Cruciate Ligament Surgery: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Complications in Canine Cranial Cruciate Ligament Surgery»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
provides revision strategies for correcting the complications associated with surgical repair techniques for cranial cruciate ligament rupture, one of the most common causes of a hind limb lameness in dogs. Presenting step-by-step instructions for numerous surgical correction techniques, this practical guide covers articular, extra-articular and osteotomy repair techniques as well as non-surgical management, physical rehabilitation, clinical decision making, and more.
The book begins with an overview of cranial cruciate ligament tear, diagnosis, and treatment goals, followed by a discussion of methods for minimizing surgical site infection and complications. Subsequent chapters describe the potential complications of a particular technique and explain how to identify, evaluate, and correct the complication. Throughout the book, hundreds of high-quality clinical photographs show the appearance of complications and demonstrate each step of the corrective procedure. This authoritative guide:
Provides step-by-step techniques for surgical corrections of common complications Emphasizes surgical decision making and specific strategies for surgical correction Contains revision strategies for identification of intra-operative complications Covers evaluation and identification of post-operative complications Features more than 400 photographs and clinical images Part of the
state-of-the-art
series,
is an invaluable resource for surgical residents, veterinary surgeons, and general practice veterinarians alike.
Complications in Canine Cranial Cruciate Ligament Surgery — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Complications in Canine Cranial Cruciate Ligament Surgery», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:

Figure 3.1 For the Levine technique, the swab is contacting the wound bed only, with sufficient application of pressure to result in exudation of fluid from the underlying tissues.
Source: Adapted from Weese JS. Wound sampling for culture and cytology. Clinician's Brief, March 2020. www.cliniciansbrief.com/article/wound‐sampling‐culture‐cytology.
As not all owners will seek veterinary care for perceived minor changes at the surgical site, another tool in our arsenal to improve detection of SSI is utilization of surveillance programs. Lack of communication between the surgical facility and primary care veterinarian can also result in underidentification of SSI rates, particularly when owners may return to their primary care veterinarian for minor complications as these may not be reported to the surgeon. Further, deficiencies in medical record quality can impact retrospective identification of SSIs.
Two recent prospective veterinary studies on postdischarge surveillance programs reported that 28–35% of identified SSIs were not documented in the medical record, leading to falsely lower SSI rates when retrospectively evaluated using medical records alone [4, 7]. Both studies carried out owner questionnaires at 30 days postoperatively and one study repeated the questionnaire at 90 days for patients having a surgical implant [4, 7]. This active surveillance approach will yield more accurate SSI information; however, these types of active surveillance approaches require time, effort, and corresponding personnel costs.
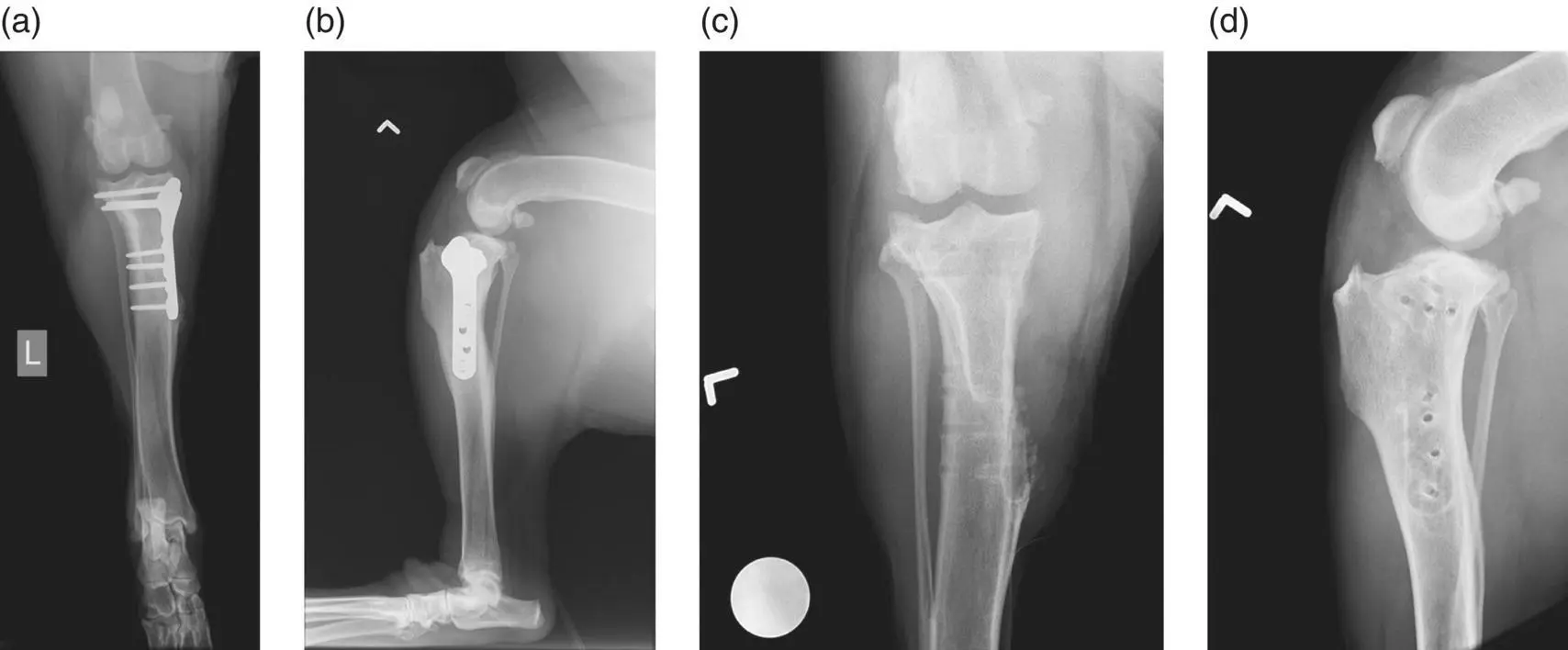
Figure 3.2 (a)A craniocaudal (CC) view of a TPLO with periosteal reaction evident at the distal aspect of the implant. (b)A lateral view of a TPLO with periosteal reaction evident at the cranial aspect of the implant, as evidenced by the increased bone density in this region corresponding to the location of periosteal reaction on the CC view. (c)A CC view following implant removal, highlighting the previously identified periosteal reaction. (d)A lateral view following implant removal, highlighting the periosteal reaction outlining the previous implant.
Developing an active surveillance protocol is an important quality control tool, but it can be challenging to achieve due to the time commitment involved [4]. However, empowering a member of the surgical team to champion an active surveillance program is highly recommended to ensure uptake and quality control. Alternatively, improving passive surveillance methods, beyond routine examination at the time of suture removal, may also be beneficial. Emphasizing the importance of SSI reporting from referring veterinarians and clients, along with defined measures of surgical site assessment to report, may help to improve the accuracy of SSI rates within your hospital [4].
More recently, electronic approaches to surveillance have been investigated. The proliferation of smartphones and email access creates the potential for easy, cost‐effective monitoring and data collection. In the future, it is likely that approaches using personal devices will become common SSI surveillance tools.
For SSIs to be appropriately identified, the use of specific criteria to define SSIs must be employed. The CDC has categorized SSIs as superficial incisional SSI, deep incisional SSI ( Figure 3.3), and organ/space SSI based on specific criteria ( Table 3.2). Recently, these categories have been redefined with regard to implant‐associated SSI, such that an implant‐associated SSI must occur within 90 days of surgery [1].

Figure 3.3 A dehisced lateral stifle incision with local erythema and purulent material present at the skin edges and present on the underlying muscle belly. This is considered to be a deep SSI.
Table 3.2 Surgical site infection (SSI) definitions.
| Surgical site infection category | Criteria |
|---|---|
| Superficial SSI | MUST:Occur within 30 daysof surgeryInvolve only the skin or subcutaneous tissuesof the incisionMust have AT LEAST one of the following: Purulent dischargefrom the incision Organism(s)identified from an aseptically collected sample Incision is reopened with purposeand organisms are identified from an aseptically collected sample AND the patient exhibits localized swelling, pain, erythema, or heatDiagnosed as an SSI by a physician |
| Deep SSI | MUST:Occur within 30 days (no implant)or 90 days (implant)Involves tissues deep to the subcutaneous tissuesMust have AT LEAST one of the following: Purulent dischargefrom the incision Incision spontaneously dehisces or is reopened with purposeAND organismsare identified from an aseptically collected sample AND the patient exhibits localized pain or pyrexiaLocal abscessformation |
| Organ/space | MUST:Occur within 30 days (no implant)or 90 days (implant)Involves any tissues deep to the fascia/muscle that was opened during surgeryMust have AT LEAST one of the following: Purulent dischargefrom a drain within the organ/space Organismsare identified from an aseptically collected sample from fluid or tissue within the organ/spaceLocal abscessformation |
3.3 Addressing Surgical Site Infections
The vast majority of SSIs occur secondary to contamination of the surgical site by commensal or pathogenic organisms arising from the patient's own microbiome [8]. The most common microorganism identified in SSIs is Staphylococcus pseudintermedius . Other common microorganisms identified include Streptococcus spp., Pseudomonas aeruginosa , and Escherichia coli . Staphylococcus pseudintermedius is an opportunistic pathogen with an ability to create a biofilm, leading to its increased virulence [9]. The ability to create a biofilm is important as it makes eradication of these SSIs more challenging. Additionally, resistance of S. pseudintermedius is on the rise, creating an even greater challenge for management of patients with SSIs [9].
Following the diagnosis of a SSI, several factors must be considered prior to determining a treatment protocol. These include the patient's overall clinical status, category of SSI (superficial, deep, organ/space), susceptibility of inciting microorganisms, presence of biofilm formation, stage of healing, availability of treatment options, and client considerations such as emotional and financial strain associated with treatment.
The vast majority of SSIs reported by category in the veterinary literature are limited to superficial or deep tissue layers, with an organ/space SSI occurring in <1% of infections [4, 10].
For superficial incisional SSIs, topical or systemic antimicrobial therapy may be sufficient. Topical therapies may include antiseptic agents such as chlorhexidine or povidone‐iodine or antimicrobial therapies such as medical‐grade honey or silver compounds. When the SSI is relatively focal or has minimal purulent discharge, topical antiseptic solutions may be used to clean the site several times daily and may result in resolution of the SSI. However, when a large portion of the wound appears to be affected or when there are large volumes of purulent discharge, topical antimicrobial therapies are best employed if the wound is reopened and explored. This allows for greater source control by lavaging the wound and removing the large microbial burden and allows topical therapies to be in direct contact with the affected tissues. Medical‐grade honey and silver ointments are often used in these scenarios. There is no evidence for antimicrobial resistance for honey, but resistance may exist for silver compounds [11]. This resistance has been demonstrated in vitro and may not be clinically applicable.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Complications in Canine Cranial Cruciate Ligament Surgery»
Представляем Вашему вниманию похожие книги на «Complications in Canine Cranial Cruciate Ligament Surgery» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.






Обсуждение, отзывы о книге «Complications in Canine Cranial Cruciate Ligament Surgery» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.