Successful Training in Gastrointestinal Endoscopy
Здесь есть возможность читать онлайн «Successful Training in Gastrointestinal Endoscopy» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Successful Training in Gastrointestinal Endoscopy
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Successful Training in Gastrointestinal Endoscopy: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Successful Training in Gastrointestinal Endoscopy»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Teaches trainee gastroenterologists the endoscopic skills needed to meet the medical training requirements to practice gastroenterology and helps clinical specialists refresh their skills to pass their recertification Successful Training in Gastrointestinal Endoscopy, Second Edition
Successful Training in Gastrointestinal Endoscopy, Second Edition
Successful Training in Gastrointestinal Endoscopy — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Successful Training in Gastrointestinal Endoscopy», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:

Figure 6.20 Looping causing perforation. In this sigmoid loop, the scope is pushing against the wall of the sigmoid colon in the direction of the arrow. One cause of perforation is due to excessive lateral pressure against the colon wall from a loop in the colon and scope.
(Copyrighted and used with permission of Mayo Foundation for Medical Education and Research.)
The key to managing colonic perforation is early recognition. Often if the perforation is caused by the scope's tip, the peritoneal cavity, organs, or serosa will be readily visible to the camera lens. When perforation occurs as a result of looping, the defect and fresh blood will commonly be identified during withdrawal. Commonly with perforations, the patient will develop increased distention of the abdomen due to free air or worsening abdominal pain either during the procedure or in recovery. If perforation is at all suspected, immediate evaluation with imaging such as an abdominal CT scan is indicated to evaluate for free peritoneal air. A CT scan can detect much smaller collections of free air than upright abdominal X‐rays and as such is preferred; however, if not available, upright abdominal X‐rays can help identify free abdominal air. If identified, immediate evaluation and likely intervention by a surgeon is required. Delay in intervention can lead to sepsis and even death. If perforation is identified during the endoscopic examination, immediate endoscopic closure is ideal followed by a single dose of broad‐spectrum antibiotic and overnight observation in the hospital for signs of peritonitis. Attempts at endoscopic closure of perforations using hemoclips or other closure devises will be discussed in Chapter 24. Endoscopic closure of defects should only be attempted by skilled endoscopists. Less commonly, perforations may be retroperitoneal (as can occur in the distal rectum) and walled off. In these cases, free air will not be identified on abdominal X‐ray. In these cases, CT scanning would be needed to identify and locate the problem. These can often be managed more conservatively with fasting and IV antibiotics with close inpatient monitoring. Occasionally, incidental radiographic findings of free air in the peritoneal cavity occur following endoscopy, yet in the absence of any clinical symptoms of perforation. The clinical significance, if any, of these findings is unclear, yet conservative management and close observation also is recommended.
Training fellows to manage perforations is difficult, as these do not occur often. The main teaching point is to never underappreciate or deny to oneself the possibility of a perforation. If there is any suspicion that a perforation has occurred, this needs to be aggressively pursued with diagnostic and therapeutic intervention as needed. In the event of a perforation, it is also paramount that the endoscopist personally stays in direct communication with the patient and family and not to simply ship the patient off to the emergency room and distance oneself from the case.
Intermediate motor skills
Loop reduction
One of the hardest skills for trainees to master is the prevention and adequate reduction of loops that develop during scope advancement. This section will address the common types and locations of loops that form and how to manage these effectively. One key concept to understand with loop formation is that of “force vectors.” Force vectors are where and in what direction the majority of the pushing force is being delivered in the colon. If a scope is perfectly straight, all of the force is being translated directly into tip advancement. If there is a 90° or greater turn, much of this force is directed at the wall of the colon on the outside part of the turn ( Figure 6.21). As the wall pushes back, some of this opposing force gets delivered forward to the scope tip, resulting in advancement, some back to the operator as resistance and some absorbed by the elastic nature of the colon wall as a loop. Reducing and straightening these loops not only removes the force against the colon wall but with correct technique can also result in prevention of recurrent loop formation and better delivery of the pushing force to the scope tip.
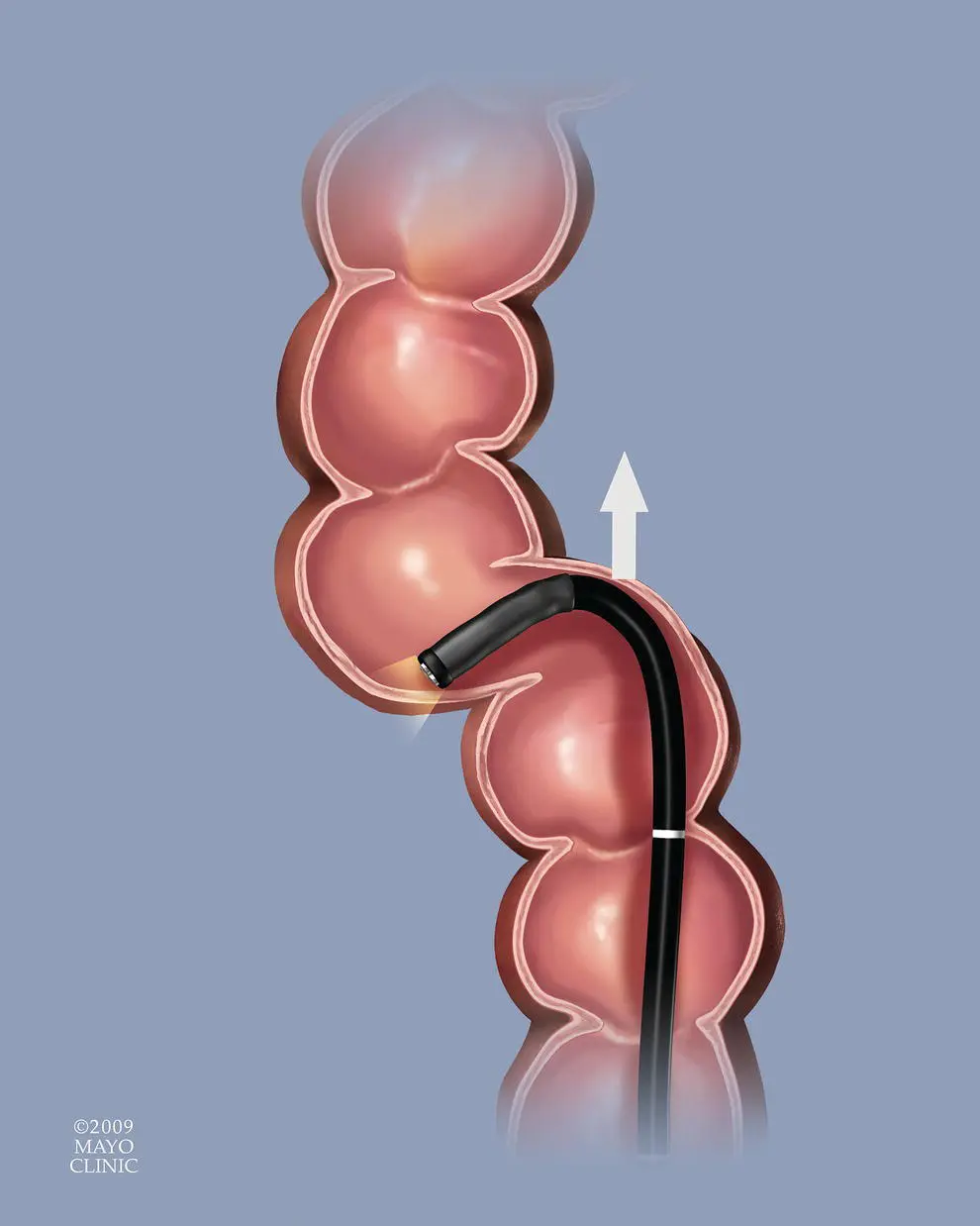
Figure 6.21 Force vector. In this illustration, the tip of the scope is deflected greater than 90° around an acute turn in the colon. In this configuration, the force vector (FV) of any attempts to advance the colon will be directed against the wall of the colon on the outside turn. This will be felt by the endoscopist as resistance to advancement or will result in looping of the scope shaft here or elsewhere in the colon.
(Copyrighted and used with permission of Mayo Foundation for Medical Education and Research.)
The sigmoid colon is the location where most loops occur. This is due to the serpentine nature of this section of colon accompanied by the fact that it is freely mobile within the abdominal cavity. The most common natural course of the sigmoid is a clockwise spiral between the rectum and descending colon. As the tip of the scope makes the first acute turn from the rectum into the sigmoid and the scope is advanced, the shaft of the scope behind the flexible scope tip tends to be pushed upward in the abdomen as the force vector of the scope is still relatively straight‐in from the anus and rectum ( Figure 6.22). This results in loss of “one‐to‐one” motion; a term meaning the scope is not advancing as much (or not at all) as the shaft of the scope is being pushed in. This extra inserted scope that is not resulting into tip advancement is instead contributing to the development of a loop. Looping can also result in “paradoxical movement” of the scope, which is when the scope tip actually moves in the opposite direction as the shaft is pushed or pulled.
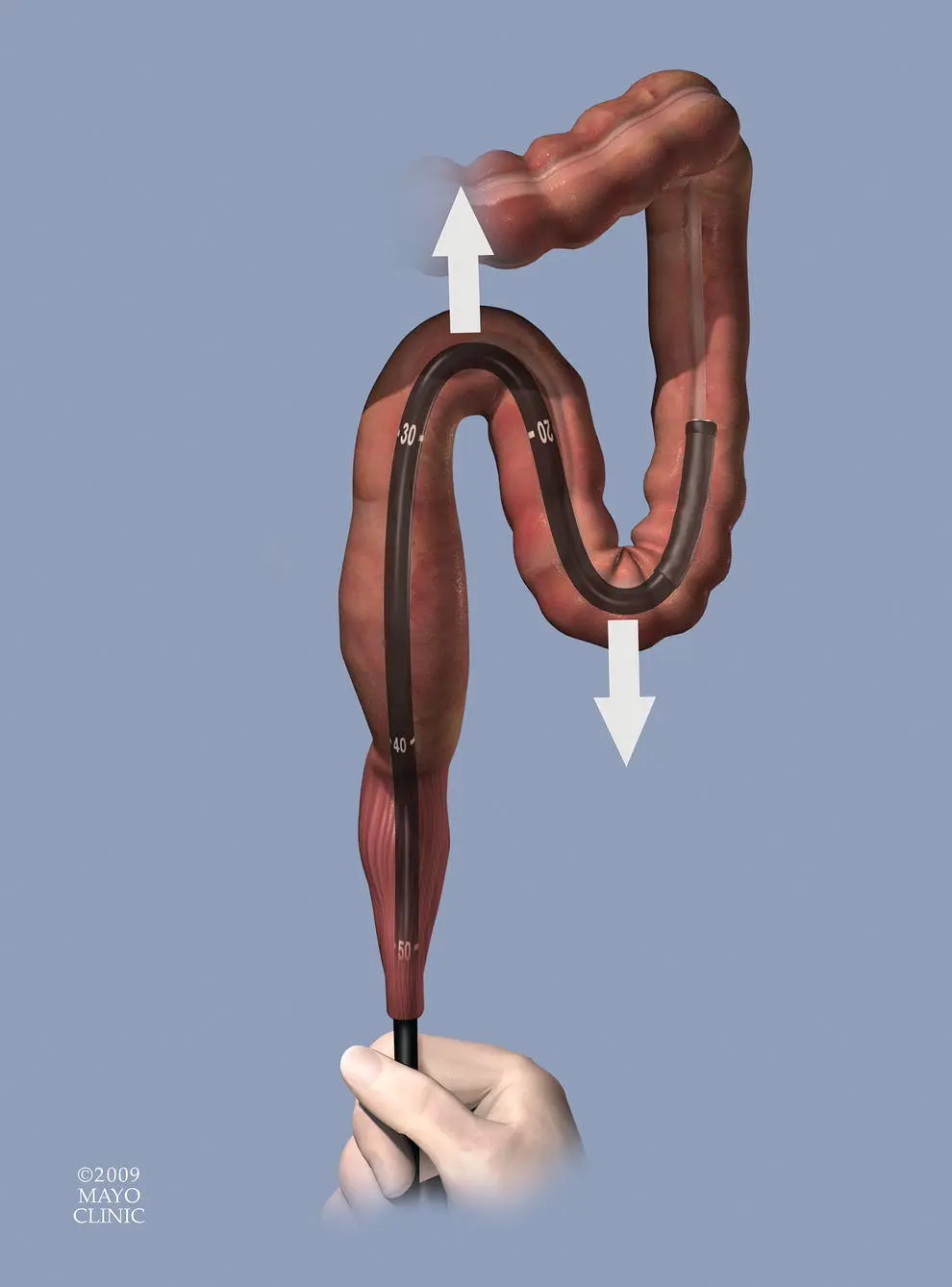
Figure 6.22 Sigmoid loop. As the scope makes multiple turns in the sigmoid colon, advancing the scope frequently results in the force being transmitted laterally against the sigmoid walls (arrows) resulting in loop formation.
(Copyrighted and used with permission of Mayo Foundation for Medical Education and Research.)
 There are three main types of loops that develop in the sigmoid colon. The “alpha‐loop” is one of the most common and is termed this because the sigmoid is looped in a counterclockwise spiral in the shape of the Greek letter of its name ( Figure 6.23) ( Video 6.5). The second most common loop is the “N‐loop” called this because it too is shaped like the letter of its name ( Figure 6.24) ( Video 6.6). This loop follows and exaggerates the normal S‐shaped spiral of the sigmoid colon. Less common than these two is the “reverse alpha‐loop” that follows a similar spiral to the alpha‐loop but the more proximal sigmoid passes behind the more distal sigmoid ( Figure 6.25) (Video 6.7). Which type of loop forms is likely due to variances in sigmoid anatomy? The method best suited for reduction of these sigmoid loops varies depending on the type of loop. In each of the loops, it is generally advisable to attempt to advance the scope beyond the splenic flexure, or other acute turn, if possible before attempting reduction. This allows the flexible portion of the scope tip to hook around this flexure and act as an anchor. This allows for greater direct force on the loop itself during reduction and torques maneuvers. Once anchored, the dials are held with the left thumb to prevent the scope tip from straightening out and slipping back into the descending colon. The two most common types of loops (alpha‐ and N‐loop) respond to slow scope withdrawal augmented by clockwise scope torque ( Figures 6.23and 6.24). During this maneuver, the tip of the scope may advance or simply remain motionless as the scope shaft is withdrawn. Clockwise torque and withdrawal of the shaft are continued until the scope tip begins to respond by starting to move backward in a one‐to‐one manner. This is evidence that the loop has been reduced. Torque is key to the maneuver as this will untwist the spiral nature of the sigmoid and create a straighter lumen if done correctly. The most common cause for failure of this technique is either failure to withdraw enough scope to re‐establish one‐to‐one motion or inadequate clockwise torque of the scope shaft during withdrawal. It is not uncommon to require 360° of torque or more during sigmoid reduction to adequately remove the spiral nature of this segment of the colon. Another cause of failure is the presence of a reverse alpha‐loop. Suspicion of this should arise if the usual clockwise maneuver repeatedly fails.
There are three main types of loops that develop in the sigmoid colon. The “alpha‐loop” is one of the most common and is termed this because the sigmoid is looped in a counterclockwise spiral in the shape of the Greek letter of its name ( Figure 6.23) ( Video 6.5). The second most common loop is the “N‐loop” called this because it too is shaped like the letter of its name ( Figure 6.24) ( Video 6.6). This loop follows and exaggerates the normal S‐shaped spiral of the sigmoid colon. Less common than these two is the “reverse alpha‐loop” that follows a similar spiral to the alpha‐loop but the more proximal sigmoid passes behind the more distal sigmoid ( Figure 6.25) (Video 6.7). Which type of loop forms is likely due to variances in sigmoid anatomy? The method best suited for reduction of these sigmoid loops varies depending on the type of loop. In each of the loops, it is generally advisable to attempt to advance the scope beyond the splenic flexure, or other acute turn, if possible before attempting reduction. This allows the flexible portion of the scope tip to hook around this flexure and act as an anchor. This allows for greater direct force on the loop itself during reduction and torques maneuvers. Once anchored, the dials are held with the left thumb to prevent the scope tip from straightening out and slipping back into the descending colon. The two most common types of loops (alpha‐ and N‐loop) respond to slow scope withdrawal augmented by clockwise scope torque ( Figures 6.23and 6.24). During this maneuver, the tip of the scope may advance or simply remain motionless as the scope shaft is withdrawn. Clockwise torque and withdrawal of the shaft are continued until the scope tip begins to respond by starting to move backward in a one‐to‐one manner. This is evidence that the loop has been reduced. Torque is key to the maneuver as this will untwist the spiral nature of the sigmoid and create a straighter lumen if done correctly. The most common cause for failure of this technique is either failure to withdraw enough scope to re‐establish one‐to‐one motion or inadequate clockwise torque of the scope shaft during withdrawal. It is not uncommon to require 360° of torque or more during sigmoid reduction to adequately remove the spiral nature of this segment of the colon. Another cause of failure is the presence of a reverse alpha‐loop. Suspicion of this should arise if the usual clockwise maneuver repeatedly fails.
Интервал:
Закладка:
Похожие книги на «Successful Training in Gastrointestinal Endoscopy»
Представляем Вашему вниманию похожие книги на «Successful Training in Gastrointestinal Endoscopy» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.










Обсуждение, отзывы о книге «Successful Training in Gastrointestinal Endoscopy» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.